

A progressive three-state model to estimate time to cancer: a likelihood-based approach
- PMID: 35761181
- PMCID: PMC9235269
- DOI: 10.1186/s12874-022-01645-2
A progressive three-state model to estimate time to cancer: a likelihood-based approach
Abstract
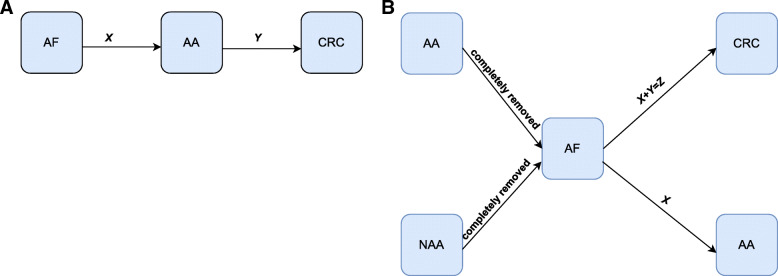
Background: To optimize colorectal cancer (CRC) screening and surveillance, information regarding the time-dependent risk of advanced adenomas (AA) to develop into CRC is crucial. However, since AA are removed after diagnosis, the time from AA to CRC cannot be observed in an ethically acceptable manner. We propose a statistical method to indirectly infer this time in a progressive three-state disease model using surveillance data.
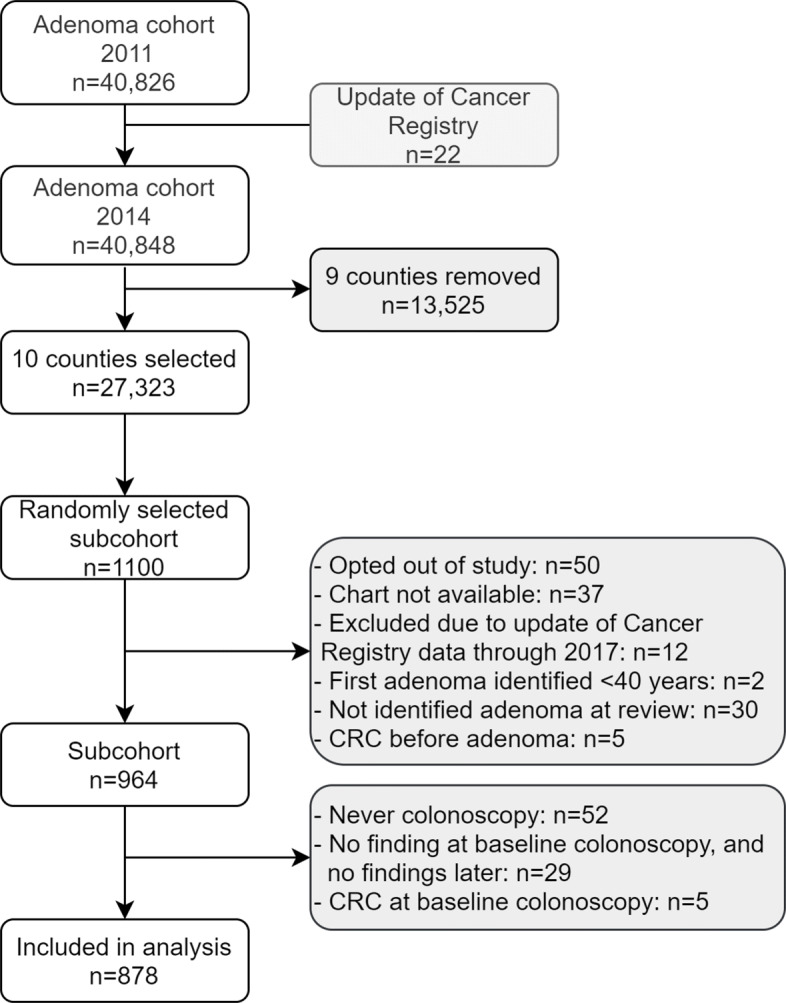
Methods: Sixteen models were specified, with and without covariates. Parameters of the parametric time-to-event distributions from the adenoma-free state (AF) to AA and from AA to CRC were estimated simultaneously, by maximizing the likelihood function. Model performance was assessed via simulation. The methodology was applied to a random sample of 878 individuals from a Norwegian adenoma cohort.
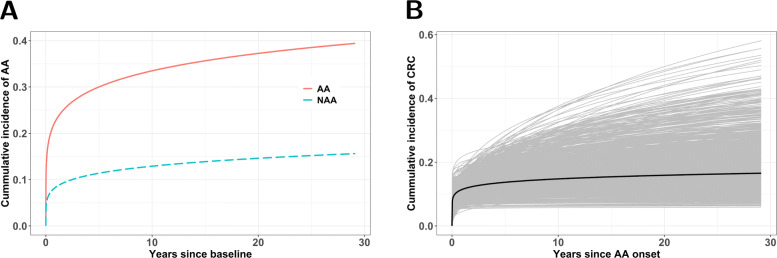
Results: Estimates of the parameters of the time distributions are consistent and the 95% confidence intervals (CIs) have good coverage. For the Norwegian sample (AF: 78%, AA: 20%, CRC: 2%), a Weibull model for both transition times was selected as the final model based on information criteria. The mean time among those who have made the transition to CRC since AA onset within 50 years was estimated to be 4.80 years (95% CI: 0; 7.61). The 5-year and 10-year cumulative incidence of CRC from AA was 13.8% (95% CI: 7.8%;23.8%) and 15.4% (95% CI: 8.2%;34.0%), respectively.
Conclusions: The time-dependent risk from AA to CRC is crucial to explain differences in the outcomes of microsimulation models used for the optimization of CRC prevention. Our method allows for improving models by the inclusion of data-driven time distributions.
Keywords: Adenoma; Adenoma surveillance; Adenoma-carcinoma sequence; Colorectal cancer; Colorectal cancer surveillance; Interval-censored data; Maximum likelihood; Progressive three-state disease model; Simulation.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Global Cancer Observatory: Cancer Today. International Agency for Research on Cancer. Lyon; 2020. https://gco.iarc.fr/today/home. Accessed 29 Jan 2021.
-
- Winawer SJ, Zauber AG, Ho MN, O’brien MJ, Gottlieb LS, Sternberg SS, Waye JD, Schapiro M, Bond JH, Panish JF, et al. Prevention of colorectal cancer by colonoscopic polypectomy. N Engl J Med. 1993;329(27):1977–81. - PubMed
-
- Mandel JS, Bond JH, Church TR, Snover DC, Bradley GM, Schuman LM, Ederer F. Reducing mortality from colorectal cancer by screening for fecal occult blood. N Engl J Med. 1993;328(19):1365–71. - PubMed
-
- Winawer SJ. Natural history of colorectal cancer. Am J Med. 1999;106(1):3–6. - PubMed
-
- Mandel JS, Church TR, Ederer F, Bond JH. Colorectal cancer mortality: effectiveness of biennial screening for fecal occult blood. J Natl Cancer Inst. 1999;91(5):434–37. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
