

First-year mortality in incident dialysis patients: results of the Peridialysis study
- PMID: 35761193
- PMCID: PMC9235232
- DOI: 10.1186/s12882-022-02852-1
First-year mortality in incident dialysis patients: results of the Peridialysis study
Abstract
Background: Controversy surrounds which factors are important for predicting early mortality after dialysis initiation (DI). We investigated associations of predialysis course and circumstances affecting planning and execution of DI with mortality following DI.
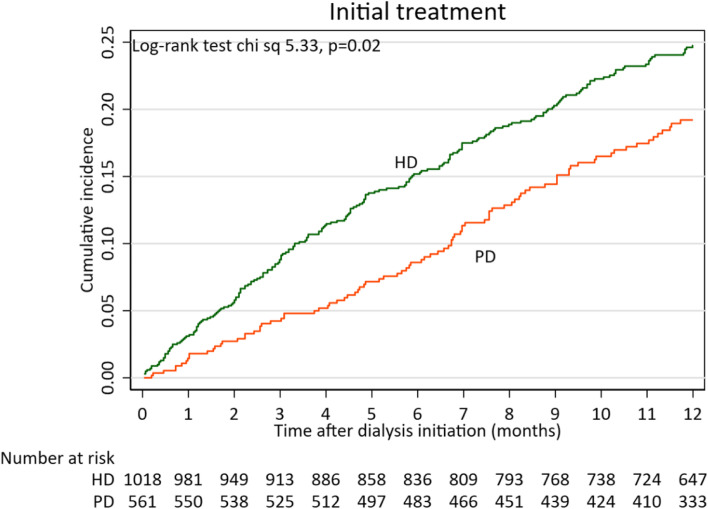
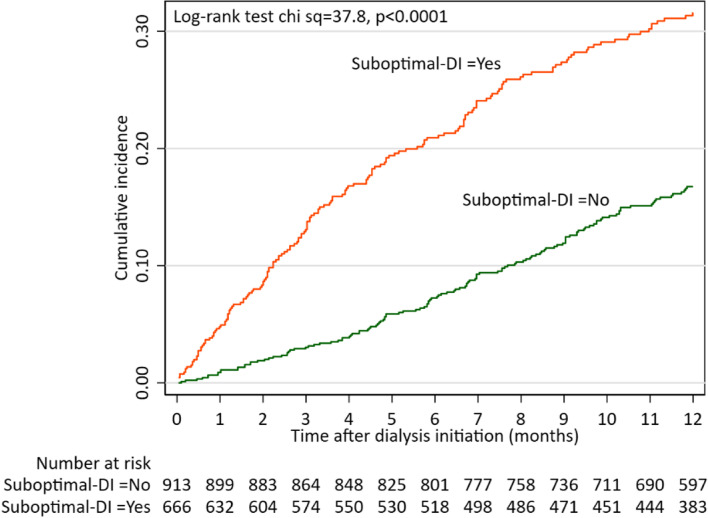
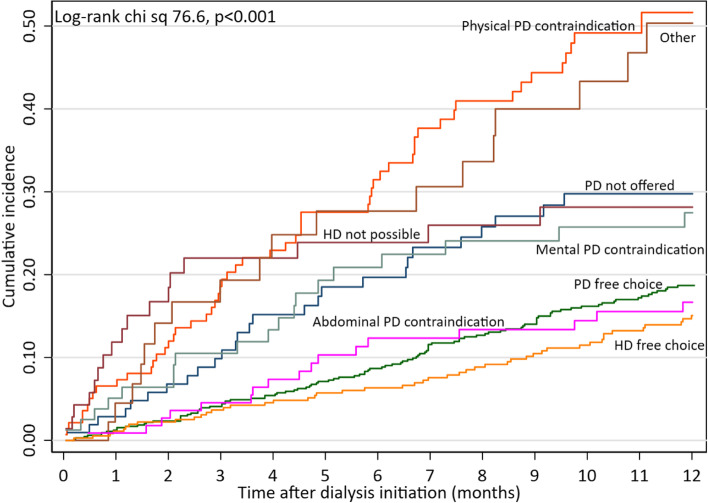
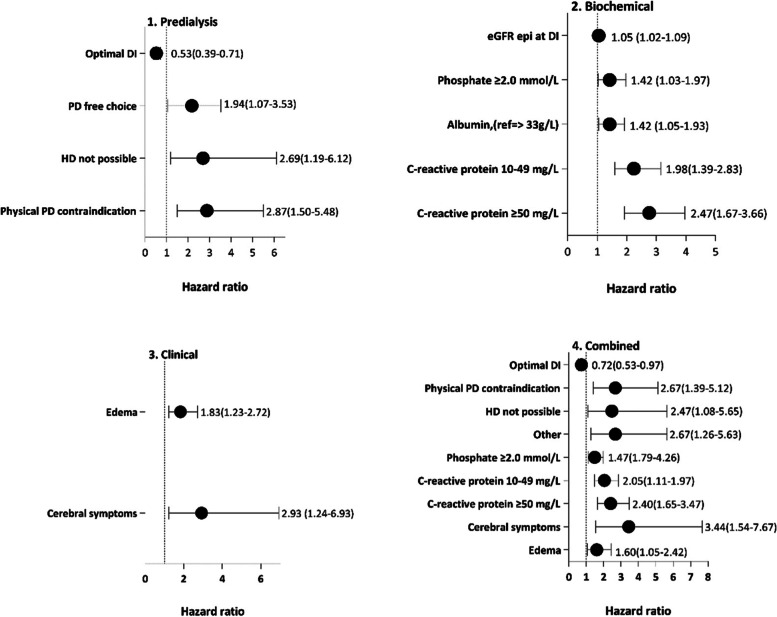
Methods: Among 1580 patients participating in the Peridialysis study, a study of causes and timing of DI, we registered features of predialysis course, clinical and biochemical data at DI, incidence of unplanned suboptimal DI, contraindications to peritoneal dialysis (PD) or hemodialysis (HD), and modality preference, actual choice, and cause of modality choice. Patients were followed for 12 months or until transplantation. A flexible parametric model was used to identify independent factors associated with all-cause mortality.
Results: First-year mortality was 19.33%. Independent factors predicting death were high age, comorbidity, clinical contraindications to PD or HD, suboptimal DI, high eGFR, low serum albumin, hyperphosphatemia, high C-reactive protein, signs of overhydration and cerebral symptoms at DI. Among 1061 (67.2%) patients who could select dialysis modality based on personal choice, 654 (61.6%) chose PD, 368 (34.7%) center HD and 39 (3.7%) home HD. The 12-months survival did not differ significantly between patients receiving PD and in-center HD.
Conclusions: First-year mortality in incident dialysis patients was in addition to high age and comorbidity, associated with clinical contraindications to PD or HD, clinical symptoms, hyperphosphatemia, inflammation, and suboptimal DI. In patients with a "free" choice of dialysis modality based on their personal preferences, PD and in-center HD led to broadly similar short-term outcomes.
Keywords: Hemodialysis; Mortality; Peritoneal dialysis; Survival analysis.
© 2022. The Author(s).
Conflict of interest statement
Bengt Lindholm is employed by Baxter Healthcare at Baxter Novum, Karolinska Institutet. None of the other authors declare any conflicts of interest.
Figures
References
-
- Pippias M, Jager KJ, Kramer A, Leivestad T, Sanchez MB, Caskey FJ, Collart F, Couchoud C, Dekker FW, Finne P, et al. The changing trends and outcomes in renal replacement therapy: data from the ERA-EDTA Registry. Nephrol Dial Transplant. 2016;31(5):831–841. - PubMed
-
- Saran R, Robinson B, Abbott KC, Bragg-Gresham J, Chen X, Gipson D, Gu H, Hirth RA, Hutton D, Jin Y, et al. US Renal Data System 2019 Annual Data Report: Epidemiology of Kidney Disease in the United States. Am J Kidney Dis. 2020;75(1 Suppl 1):A6–A7. - PubMed
-
- van Walraven C, Manuel DG, Knoll G. Survival trends in ESRD patients compared with the general population in the United States. Am J Kidney Dis. 2014;63(3):491–499. - PubMed
-
- McIntyre CW, Rosansky SJ. Starting dialysis is dangerous: how do we balance the risk? Kidney Int. 2012;82(4):382–387. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
