

Polygenic risk scores indicate extreme ages at onset of breast cancer in female BRCA1/2 pathogenic variant carriers
- PMID: 35761208
- PMCID: PMC9238030
- DOI: 10.1186/s12885-022-09780-1
Polygenic risk scores indicate extreme ages at onset of breast cancer in female BRCA1/2 pathogenic variant carriers
Abstract
Background: Clinical management of women carrying a germline pathogenic variant (PV) in the BRCA1/2 genes demands for accurate age-dependent estimators of breast cancer (BC) risks, which were found to be affected by a variety of intrinsic and extrinsic factors. Here we assess the contribution of polygenic risk scores (PRSs) to the occurrence of extreme phenotypes with respect to age at onset, namely, primary BC diagnosis before the age of 35 years (early diagnosis, ED) and cancer-free survival until the age of 60 years (late/no diagnosis, LD) in female BRCA1/2 PV carriers.
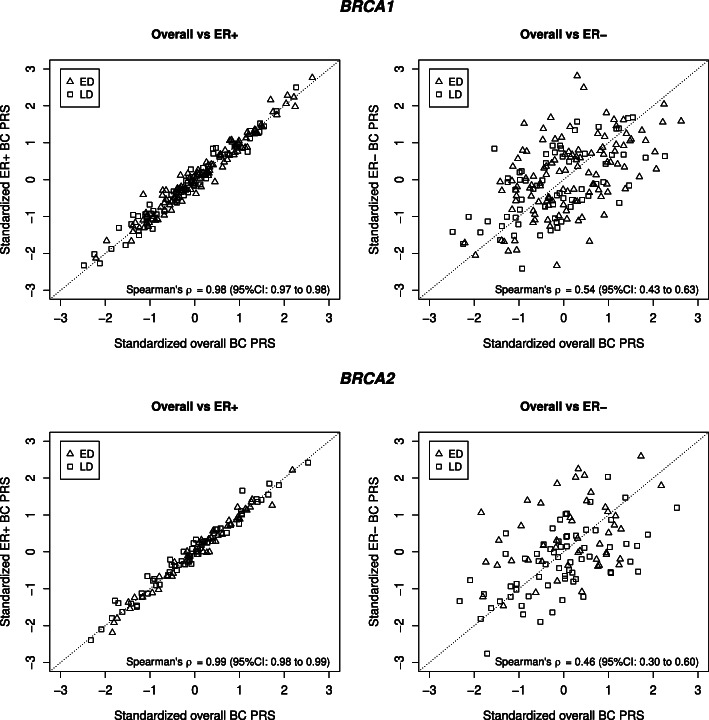
Methods: Overall, estrogen receptor (ER)-positive, and ER-negative BC PRSs as developed by Kuchenbaecker et al. for BC risk discrimination in female BRCA1/2 PV carriers were employed for PRS computation in a curated sample of 295 women of European descent carrying PVs in the BRCA1 (n=183) or the BRCA2 gene (n=112), and did either fulfill the ED criteria (n=162, mean age at diagnosis: 28.3 years, range: 20 to 34 years) or the LD criteria (n=133). Binomial logistic regression was applied to assess the association of standardized PRSs with either ED or LD under adjustment for patient recruitment criteria for germline testing and localization of BRCA1/2 PVs in the corresponding BC or ovarian cancer (OC) cluster regions.
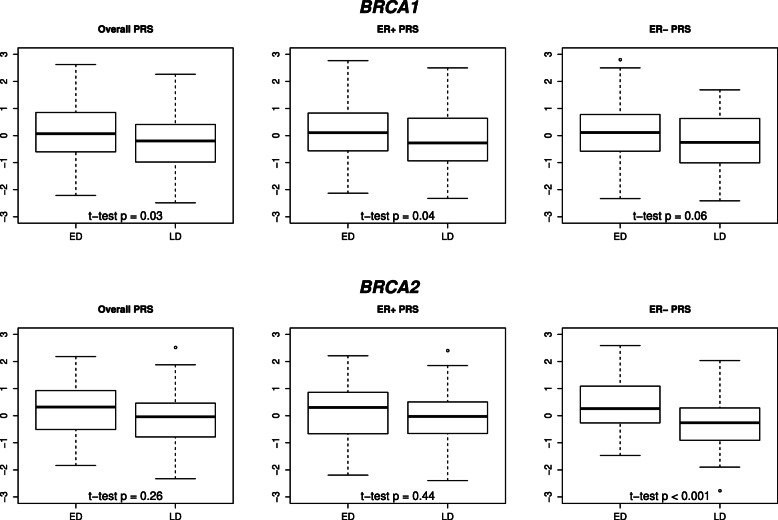
Results: For BRCA1 PV carriers, the standardized overall BC PRS displayed the strongest association with ED (odds ratio (OR) = 1.62; 95% confidence interval (CI): 1.16-2.31, p<0.01). Additionally, statistically significant associations of selection for the patient recruitment criteria for germline testing and localization of pathogenic PVs outside the BRCA1 OC cluster region with ED were observed. For BRCA2 PV carriers, the standardized PRS for ER-negative BC displayed the strongest association (OR = 2.27, 95% CI: 1.45-3.78, p<0.001).
Conclusions: PRSs contribute to the development of extreme phenotypes of female BRCA1/2 PV carriers with respect to age at primary BC diagnosis. Construction of optimized PRS SNP sets for BC risk stratification in BRCA1/2 PV carriers should be the task of future studies with larger, well-defined study samples. Furthermore, our results provide further evidence, that localization of PVs in BC/OC cluster regions might be considered in BC risk calculations for unaffected BRCA1/2 PV carriers.
Keywords: BRCA1; BRCA2; Breast cancer; PRS; Polygenic risk score; Risk assessment.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Kuchenbaecker KB, Hopper JL, Barnes DR, Phillips K-A, Mooij TM, Roos-Blom M-J, Jervis S, Van Leeuwen FE, Milne RL, Andrieu N, et al. Risks of breast, ovarian, and contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. Jama. 2017;317(23):2402–16. doi: 10.1001/jama.2017.7112. - DOI - PubMed
MeSH terms
Substances
Grants and funding
- 01GY1901/Federal Ministry of Education and Research (BMBF), Germany
- 01GY1901/Federal Ministry of Education and Research (BMBF), Germany
- 01GY1901/Federal Ministry of Education and Research (BMBF), Germany
- 01GY1901/Federal Ministry of Education and Research (BMBF), Germany
- #110837, #70111850/German Cancer Aid
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
