

"Everything has been tried and his heart can't recover…": A Descriptive Review of "Do Everything!" in the Archive of Ontario Consent and Capacity Board
- PMID: 35761229
- PMCID: PMC9237977
- DOI: 10.1186/s12910-022-00796-7
"Everything has been tried and his heart can't recover…": A Descriptive Review of "Do Everything!" in the Archive of Ontario Consent and Capacity Board
Abstract
Background: In end-of-life situations, the phrase "do everything" is sometimes invoked by physicians, patients, or substitute decision-makers (SDM), though its meaning is ambiguous. We examined instances of the phrase "do everything" in the archive of the Ontario Consent and Capacity Board (CCB) in Canada, a tribunal with judicial authority to adjudicate physician-patient conflicts in order to explore its potential meanings.
Methods: We systematically searched the CCB's online public archive from its inception to 2018 for any references to "do everything" in the context of critical care medicine and end-of-life care. Two independent assessors reviewed decisions, collected characteristics, and identified key themes.
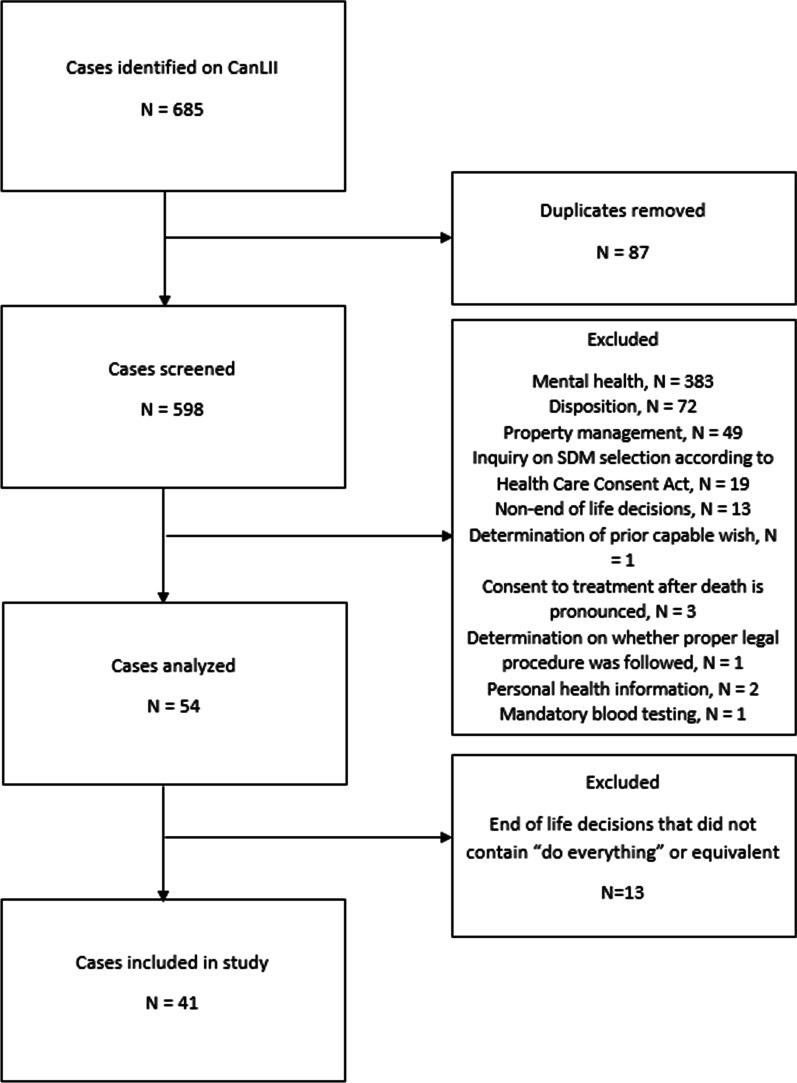
Results: Of 598 cases in the archive, 41 referred to "do everything" in end-of-life situations. The phrase was overwhelmingly invoked by SDMs (38/41, 93%), typically to advocate for life-prolonging measures that contradicted physician advice. Physicians generally related "doing everything" to describe the interventions they had already performed (3/41, 7%), using it to recommend focusing on patients' quality of life. SDMs were generally reluctant to accept death, whereas physicians found prolonging life at all costs to be morally distressing. The CCB did not interpret appeals to "do everything" legally but followed existing laws by deferring to patients' prior wishes whenever known, or to concepts of "best interests" when not. The CCB generally recommended against life-prolonging measures in these cases (26/41, 63%), focusing on patients' "well-being" and "best interests."
Conclusions: In this unique sample of cases involving conflict surrounding resuscitation and end-of-life care, references to "do everything" highlighted conflicts over quantity versus quality of life. These appeals were associated with signs of cognitive distress on the behalf of SDMs who were facing the prospect of a patient's death, whereas physicians identified moral distress related to the prolongation of patients' suffering through their use of life-sustaining interventions. This divergence in perspectives on death versus suffering was consistently the locus of conflict. These findings support the importance of tools such as the Serious Illness Conversation Guide that can be used by physicians to direct conversations on the patients' goals, wishes, trade-offs, and to recommend a treatment plan that may include palliative care.
Trial registration: Not applicable.
Keywords: Bioethics; Communication; Critical care; Goals of care; Palliative care.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Zitter JN. When “Doing everything” is way too much. Opinionator. 2015 [cited 2022 Mar 28]. Available from: https://opinionator.blogs.nytimes.com/2015/02/07/when-doing-everything-i...
-
- Canada SC of. Cuthbertson v. Rasouli, 2013 SCC 53, [2013] 3 S.C.R. 341; 2013 Oct 18; [cited 2016 April 13]. 2001 [cited 2022 Mar 28]. Available from: https://scc-csc.lexum.com/scc-csc/scc-csc/en/item/13290/index.do
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
