

Fully endoscopic microvascular decompression for hemifacial spasm
- PMID: 35761812
- PMCID: PMC9214605
- DOI: 10.3892/etm.2022.11410
Fully endoscopic microvascular decompression for hemifacial spasm
Abstract
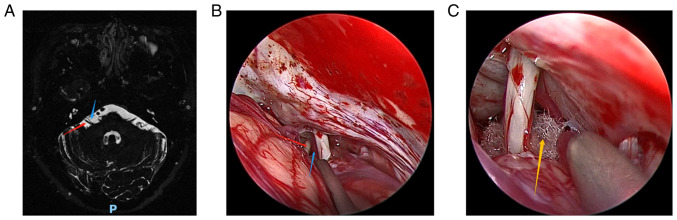
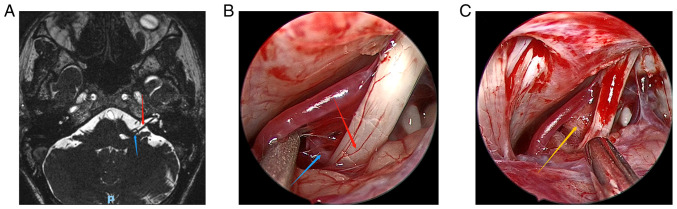
With the rapid development of endoscopic technology, fully endoscopic microvascular decompression (MVD) has been widely used in the treatment of hemifacial spasm (HFS), and has achieved good effect. The present study reviewed 5 cases of HFS treated by fully endoscopic MVD. After fully endoscopic MVD, the symptom of facial involuntary twitching was relieved in each of the 5 patients with an effective rate of 100%. Among the cases, 4 had no postoperative complications, such as cranial nerve dysfunction, and cerebellar or brainstem injury, while 1 patient had postoperative aseptic meningitis and recovered after follow-up treatment. In these 5 cases of MVD, endoscopy played an important role in identifying the offending blood vessels, which is of great significance to improve the surgical effect and safety. Furthermore, the postoperative effects showed that endoscopy has certain potential and advantages in MVD. Therefore, fully endoscopic MVD is also a feasible method for the treatment of HFS.
Keywords: endoscopy; hemifacial spasm; microvascular decompression.
Copyright: © Jiang et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
-
- Teton ZE, Blatt D, Holste K, Raslan AM, Burchiel KJ. Utilization of 3D imaging reconstructions and assessment of symptom-free survival after microvascular decompression of the facial nerve in hemifacial spasm. J Neurosurg: 1-8, 2019 (Epub ahead of print). - PubMed
LinkOut - more resources
Full Text Sources