

Blood Flow Restriction Therapy Preserves Lower Extremity Bone and Muscle Mass After ACL Reconstruction
- PMID: 35762124
- PMCID: PMC10170230
- DOI: 10.1177/19417381221101006
Blood Flow Restriction Therapy Preserves Lower Extremity Bone and Muscle Mass After ACL Reconstruction
Abstract
Background: Muscle atrophy is common after an injury to the knee and anterior cruciate ligament reconstruction (ACLR). Blood flow restriction therapy (BFR) combined with low-load resistance exercise may help mitigate muscle loss and improve the overall condition of the lower extremity (LE).
Purpose: To determine whether BFR decreases the loss of LE lean mass (LM), bone mass, and bone mineral density (BMD) while improving function compared with standard rehabilitation after ACLR.
Study design: Randomized controlled clinical trial.
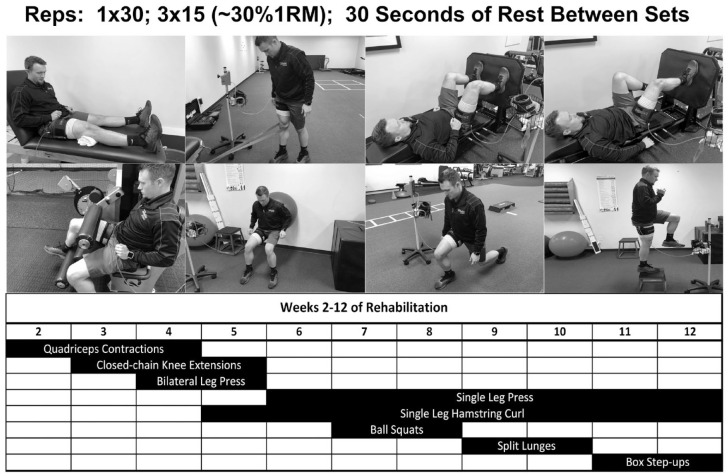
Methods: A total of 32 patients undergoing ACLR with bone-patellar tendon-bone autograft were randomized into 2 groups (CONTROL: N = 15 [male = 7, female = 8; age = 24.1 ± 7.2 years; body mass index [BMI] = 26.9 ± 5.3 kg/m2] and BFR: N = 17 [male = 12, female = 5; age = 28.1 ± 7.4 years; BMI = 25.2 ± 2.8 kg/m2]) and performed 12 weeks of postsurgery rehabilitation with an average follow-up of 2.3 ± 1.0 years. Both groups performed the same rehabilitation protocol. During select exercises, the BFR group exercised under 80% arterial occlusion of the postoperative limb (Delfi tourniquet system). BMD, bone mass, and LM were measured using DEXA (iDXA, GE) at presurgery, week 6, and week 12 of rehabilitation. Functional measures were recorded at week 8 and week 12. Return to sport (RTS) was defined as the timepoint at which ACLR-specific objective functional testing was passed at physical therapy. A group-by-time analysis of covariance followed by a Tukey's post hoc test were used to detect within- and between-group changes. Type I error; α = 0.05.
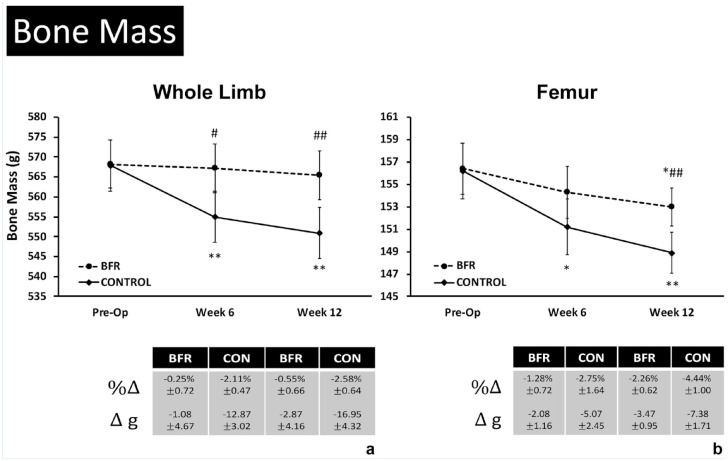
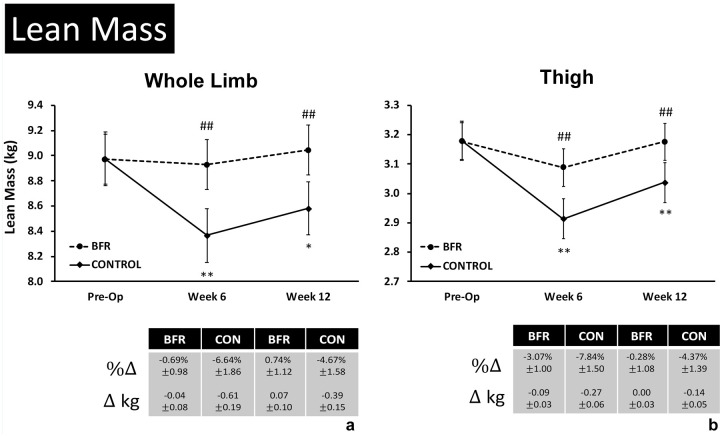
Results: Compared with presurgery, only the CONTROL group experienced decreases in LE-LM at week 6 (-0.61 ± 0.19 kg, -6.64 ± 1.86%; P < 0.01) and week 12 (-0.39 ± 0.15 kg, -4.67 ± 1.58%; P = 0.01) of rehabilitation. LE bone mass was decreased only in the CONTROL group at week 6 (-12.87 ± 3.02 g, -2.11 ± 0.47%; P < 0.01) and week 12 (-16.95 ± 4.32 g,-2.58 ± 0.64%; P < 0.01). Overall, loss of site-specific BMD was greater in the CONTROL group (P < 0.05). Only the CONTROL group experienced reductions in proximal tibia (-8.00 ± 1.10%; P < 0.01) and proximal fibula (-15.0±2.50%,P < 0.01) at week 12 compared with presurgery measures. There were no complications. Functional measures were similar between groups. RTS time was reduced in the BFR group (6.4 ± 0.3 months) compared with the CONTROL group (8.3 ± 0.5 months; P = 0.01).
Conclusion: After ACLR, BFR may decrease muscle and bone loss for up to 12 weeks postoperatively and may improve time to RTS with functional outcomes comparable with those of standard rehabilitation.
Keywords: ACL; anterior cruciate ligament; blood flow restriction; rehabilitation.
Conflict of interest statement
The authors report no potential conflicts of interest in the development and publication of this article.
Figures



References
-
- Abe T, Kearns CF, Sato Y. Muscle size and strength are increased following walk training with restricted venous blood flow from the leg muscle, Kaatsu-walk training. J Appl Physiol. 2006;100:1460-1466. - PubMed
-
- Abe T, Sakamaki M, Fujita S, et al.. Effects of low-intensity walk training with restricted leg blood flow on muscle strength and aerobic capacity in older adults. J Ger Phys Ther. 2010;33:34-40. - PubMed
-
- Abe T, Yasuda T, Midorikawa T, et al.. Skeletal muscle size and circulating IGF-1 are increased after two weeks of twice daily “KAATSU” resistance training. Int J KAATSU Train Res. 2005;1:6-12.
-
- Anderson AW, Smith JJ. Proximal tibial fracture after patellar tendon autograft for ipsilateral ACL reconstruction. J Knee Surg. 2009;22:142-144. - PubMed
-
- Ardern CL, Webster KE, Taylor NF, Feller JA. Return to the preinjury level of competitive sport after anterior cruciate ligament reconstruction surgery: two-thirds of patients have not returned by 12 months after surgery. Am J Sports Med. 2011;39:538-543. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
