

Brain metastases: A Society for Neuro-Oncology (SNO) consensus review on current management and future directions
- PMID: 35762249
- PMCID: PMC9527527
- DOI: 10.1093/neuonc/noac118
Brain metastases: A Society for Neuro-Oncology (SNO) consensus review on current management and future directions
Abstract
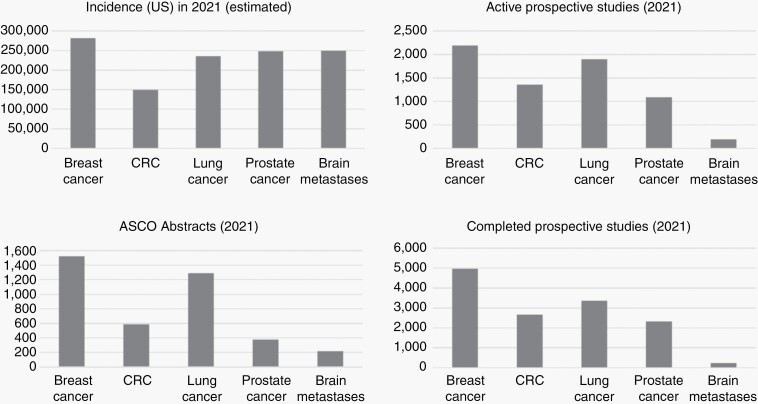
Brain metastases occur commonly in patients with advanced solid malignancies. Yet, less is known about brain metastases than cancer-related entities of similar incidence. Advances in oncologic care have heightened the importance of intracranial management. Here, in this consensus review supported by the Society for Neuro-Oncology (SNO), we review the landscape of brain metastases with particular attention to management approaches and ongoing efforts with potential to shape future paradigms of care. Each coauthor carried an area of expertise within the field of brain metastases and initially composed, edited, or reviewed their specific subsection of interest. After each subsection was accordingly written, multiple drafts of the manuscript were circulated to the entire list of authors for group discussion and feedback. The hope is that the these consensus guidelines will accelerate progress in the understanding and management of patients with brain metastases, and highlight key areas in need of further exploration that will lead to dedicated trials and other research investigations designed to advance the field.
Keywords: brain metastases; consensus; expert; guidelines; recommendations; treatment.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Nayak L, Lee EQ, Wen PY. Epidemiology of brain metastases. Curr Oncol Rep. 2012; 14(1):48–54. - PubMed
-
- Barnholtz-Sloan JS, Sloan AE, Davis FG, et al. Incidence proportions of brain metastases in patients diagnosed (1973 to 2001) in the Metropolitan Detroit Cancer Surveillance System. J Clin Oncol. 2004; 22(14):2865–2872. - PubMed
-
- Achrol AS, Rennert RC, Anders C, et al. Brain metastases. Nat Rev Dis Primers. 2019; 5(1):5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
