

Mid-term Surgery Outcomes in Patients With COVID-19: Results From a Nationwide Analysis
- PMID: 35762608
- PMCID: PMC9794632
- DOI: 10.1097/SLA.0000000000005515
Mid-term Surgery Outcomes in Patients With COVID-19: Results From a Nationwide Analysis
Abstract
Objective: Determine mid-term postoperative outcomes among coronavirus disease 2019 (COVID-19)-positive (+) patients compared with those who never tested positive before surgery.
Background: COVID-19 is thought to be associated with prohibitively high rates of postoperative complications. However, prior studies have only evaluated 30-day outcomes, and most did not adjust for demographic, clinical, or procedural characteristics.
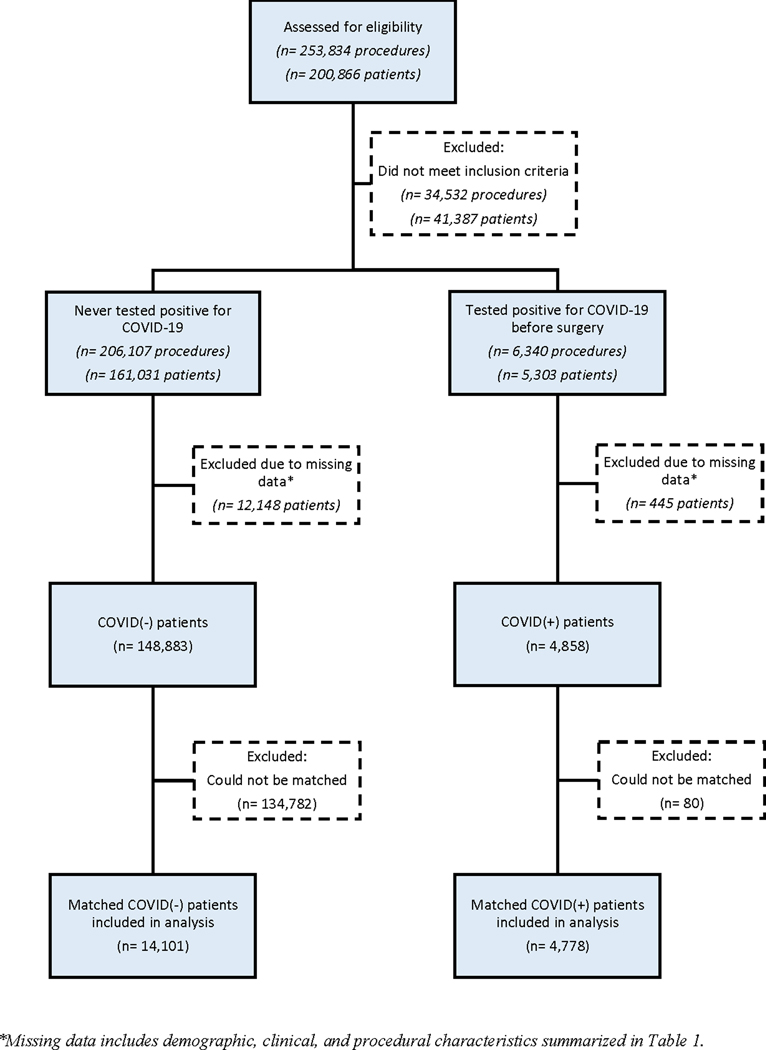
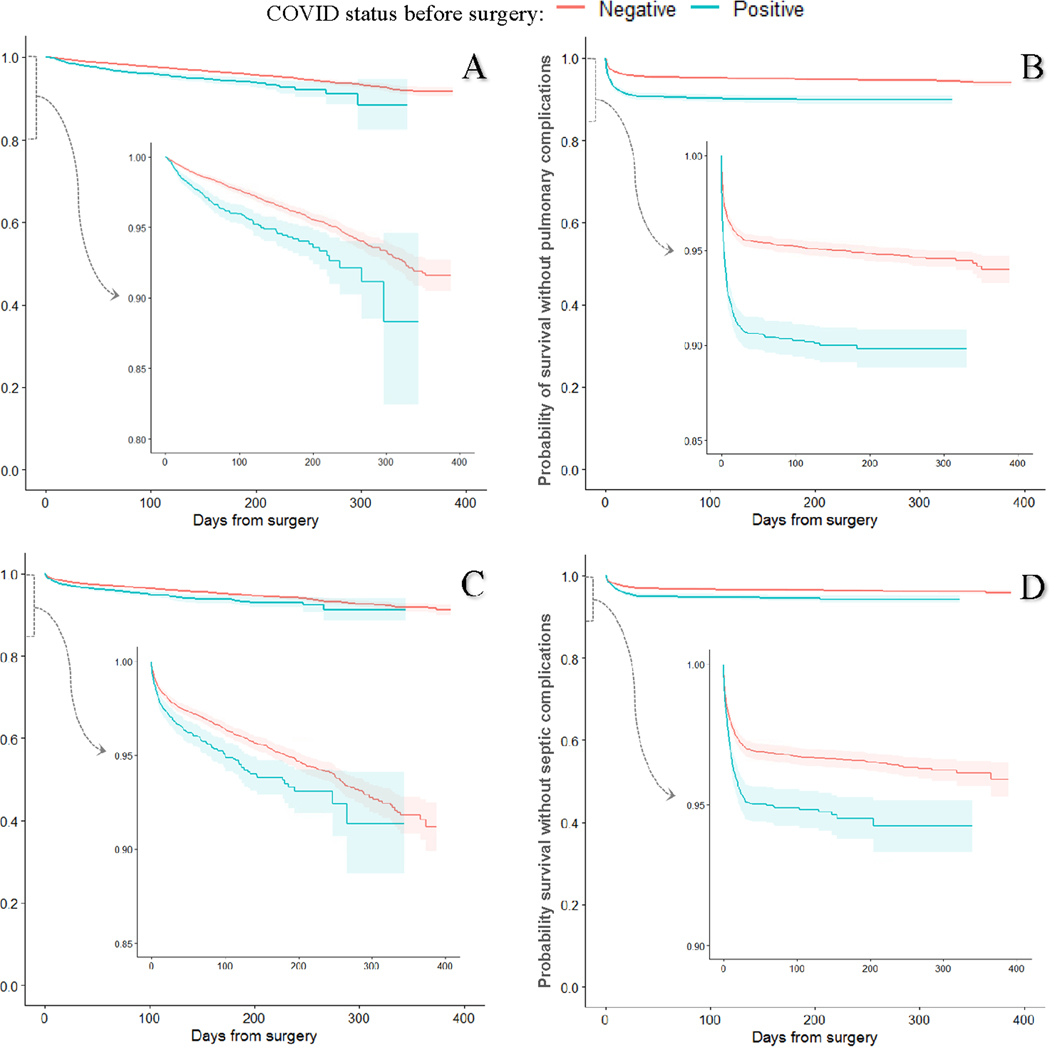
Methods: We analyzed data from surgeries performed at all Veterans Affairs hospitals between March 2020 and 2021. Kaplan-Meier curves compared trends in mortality and Cox proportional hazards models estimated rates of mortality and pulmonary, thrombotic, and septic postoperative complications between patients with a positive preoperative severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) test [COVID (+)] and propensity score-matched COVID-negative (-) patients.
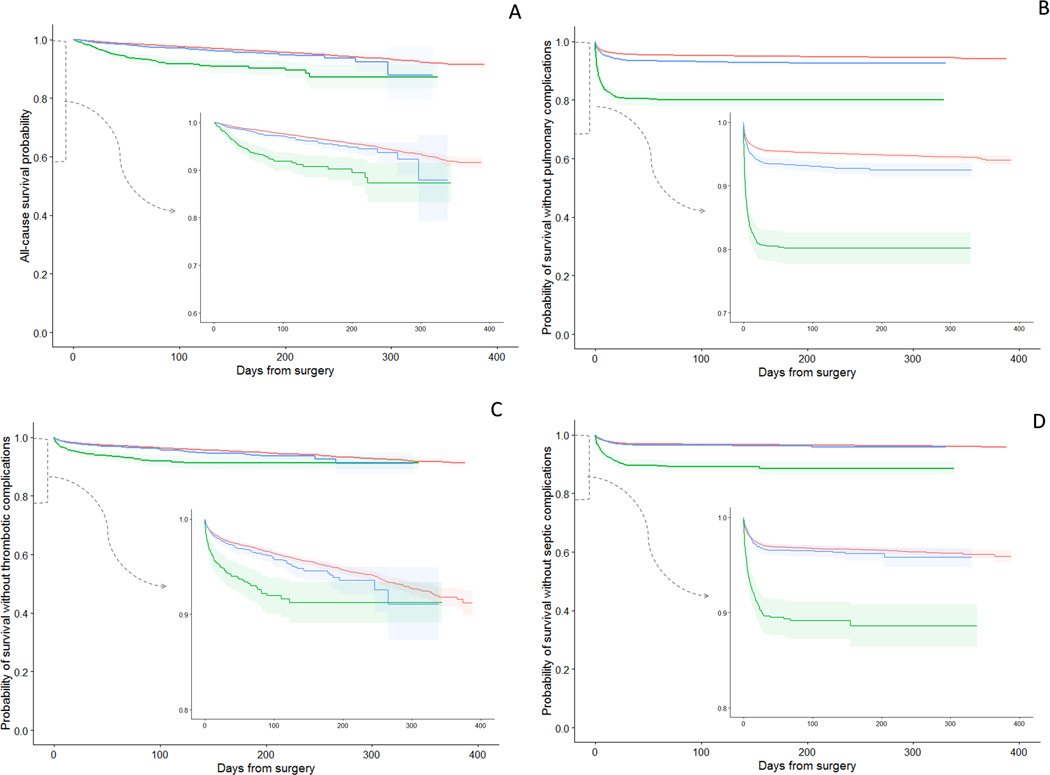
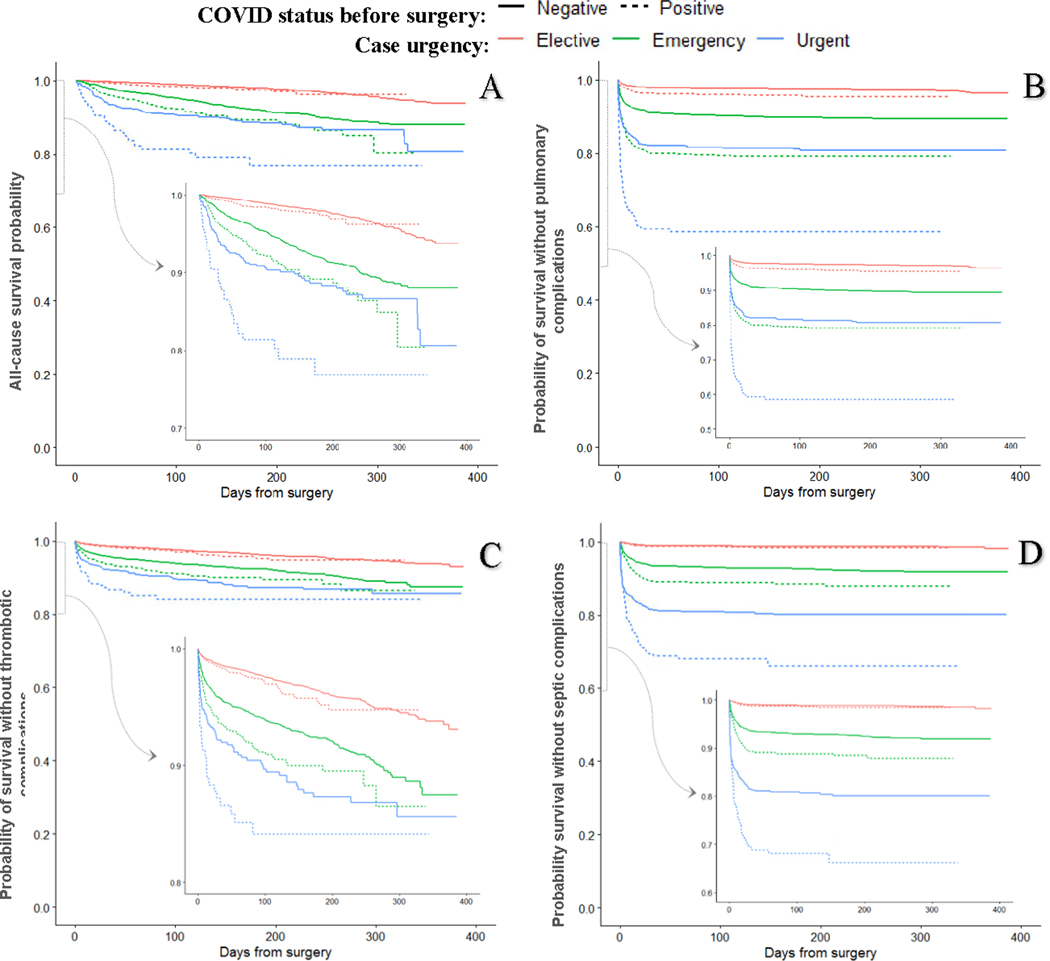
Results: Of 153,741 surgical patients, 4778 COVID (+) were matched to 14,101 COVID (-). COVID (+) status was associated with higher postoperative mortality ( P <0.0001) with a 6-month survival of 94.2% (95% confidence interval: 93.2-95.2) versus 96.0% (95% confidence interval: 95.7.0-96.4) in COVID (-). The highest mortality was in the first 30 postoperative days. Hazards for mortality and postoperative complications in COVID (+) decreased with increasing time between testing COVID (+) and date of surgery. COVID (+) patients undergoing elective surgery had similar rates of mortality, thrombotic and septic complications, but higher rates of pulmonary complications than COVID (-) patients.
Conclusions: This is the first report of mid-term outcomes among COVID-19 patients undergoing surgery. COVID-19 is associated with decreased overall and complication-free survival primarily in the early postoperative period, delaying surgery by 5 weeks or more reduces risk of complications. Case urgency has a multiplicative effect on short-term and long-term risk of postoperative mortality and complications.
Copyright © 2022 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
