

Is it time to consider population screening for fracture risk in postmenopausal women? A position paper from the International Osteoporosis Foundation Epidemiology/Quality of Life Working Group
- PMID: 35763133
- PMCID: PMC9239944
- DOI: 10.1007/s11657-022-01117-6
Is it time to consider population screening for fracture risk in postmenopausal women? A position paper from the International Osteoporosis Foundation Epidemiology/Quality of Life Working Group
Abstract
The IOF Epidemiology and Quality of Life Working Group has reviewed the potential role of population screening for high hip fracture risk against well-established criteria. The report concludes that such an approach should strongly be considered in many health care systems to reduce the burden of hip fractures.
Introduction: The burden of long-term osteoporosis management falls on primary care in most healthcare systems. However, a wide and stable treatment gap exists in many such settings; most of which appears to be secondary to a lack of awareness of fracture risk. Screening is a public health measure for the purpose of identifying individuals who are likely to benefit from further investigations and/or treatment to reduce the risk of a disease or its complications. The purpose of this report was to review the evidence for a potential screening programme to identify postmenopausal women at increased risk of hip fracture.
Methods: The approach took well-established criteria for the development of a screening program, adapted by the UK National Screening Committee, and sought the opinion of 20 members of the International Osteoporosis Foundation's Working Group on Epidemiology and Quality of Life as to whether each criterion was met (yes, partial or no). For each criterion, the evidence base was then reviewed and summarized.
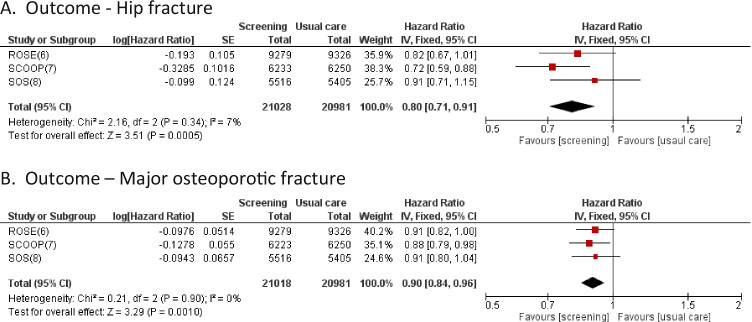
Results and conclusion: The report concludes that evidence supports the proposal that screening for high fracture risk in primary care should strongly be considered for incorporation into many health care systems to reduce the burden of fractures, particularly hip fractures. The key remaining hurdles to overcome are engagement with primary care healthcare professionals, and the implementation of systems that facilitate and maintain the screening program.
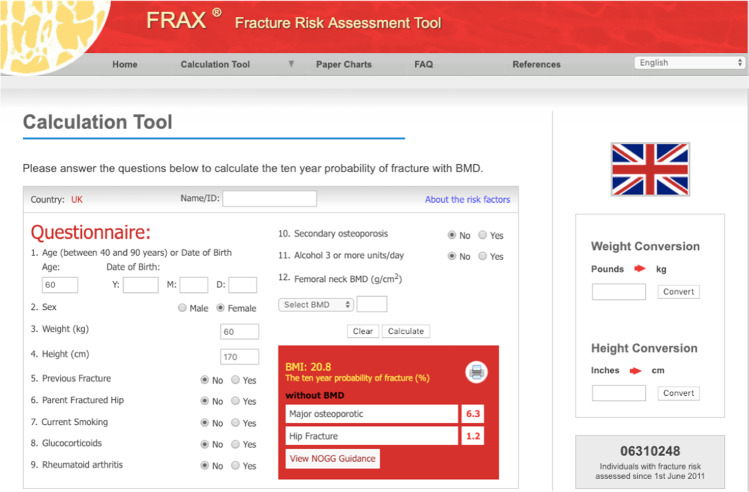
Keywords: Cost-effectiveness; FRAX; Fracture risk; Screening; Treatment.
© 2022. The Author(s).
Conflict of interest statement
E.V.M reports consultant/advisor fees, speaker honoraria and or, research funding from AgNovos, Amgen, Consilient Healthcare, Fresenius Kabi, Gedeon Richter, Internis, Lilly, Novartis, ObsEva, Synexus and UCB, all outside the submitted work. E.M.C. reports lecture fees and travel support from Eli Lilly, Pfizer and UCB, outside the submitted work. N.C.H. reports personal fees, consultancy, lecture fees and honoraria from Alliance for Better Bone Health, AMGEN, MSD, Eli Lilly, UCB, Kyowa Kirin, Servier, Shire, Consilient Healthcare and Internis Pharma, outside the submitted work. J.A.K. reports a grant from UCB, outside the submitted work. He is the architect of FRAX® but has no financial interest. C.C. reports personal fees from ABBH, Amgen, Eli Lilly, GSK, Medtronic, Merck, Novartis, Pfizer, Roche, Servier and Takeda, outside the submitted work. B.A. reports grants and personal fees from UCB, personal fees from Amgen, grants from Novartis, grants and personal fees from Pharma-cosmos, grants and personal fees from Kyowa Kirin, personal fees for Gedeon Richter outside the submitted work. BA also serves on the NovoNordisk Foundation Grants Committee on Endocrinology and Metabolism. M.L. reports lecture fees from Amgen, Astellas, Lilly, Meda, Renapharma and UCB Pharma and consulting fees from Amgen, Radius Health, UCB Pharma, Renapharma and Consilient Health, outside the submitted work. D.P-A. reports institutional receipt of speaker fees from AMGEN and UCB Biopharma; consultancy fees from UCB Biopharma; research grants from UCB, Amgen, and Les Laboratoires Servier, all outside of the submitted work. J. A. reports grants and personal fees from Amgen outside the submitted work, grants from Radius and has been an advisor to Gilead and is part of their speaker’s bureau, outside the submitted work. F.B. is employed and is a shareholder in Quantify Research, a health economic research consultancy, outside of the submitted work. O.B. reports grant support from IBSA, MSD, Nutraveris, Novartis, Pfizer, Rottapharm, Servier and Theramex; consulting or lecture fees from Bayer, Genevrier, IBSA, Rottapharm, Servier, SMB and TRB Chemedica; all outside the submitted work. All other authors have no relevant conflicts of interest in relation to the submitted work.
Figures
References
-
- Wilson JMG, Jungner G (1968) Principles and practice of screening for disease. World Health Organization https://apps.who.int/iris/handle/10665/37650. Accessed 18 Aug 2021
-
- Shepstone L, Fordham R, Lenaghan E, et al. A pragmatic randomised controlled trial of the effectiveness and cost-effectiveness of screening older women for the prevention of fractures: rationale, design and methods for the SCOOP study. Osteoporos Int. 2012;23:2507–2515. doi: 10.1007/s00198-011-1876-7. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
- MC_UP_A620_1015/MRC_/Medical Research Council/United Kingdom
- MC_UU_12011/2/MRC_/Medical Research Council/United Kingdom
- 19583/VAC_/Versus Arthritis/United Kingdom
- MC_UU_12011/1/MRC_/Medical Research Council/United Kingdom
- G0400491/MRC_/Medical Research Council/United Kingdom
- MC_U147585824/MRC_/Medical Research Council/United Kingdom
- MC_U147585827/MRC_/Medical Research Council/United Kingdom
- MC_PC_21000/MRC_/Medical Research Council/United Kingdom
- MC_U147585819/MRC_/Medical Research Council/United Kingdom
- MC_PC_21003/MRC_/Medical Research Council/United Kingdom
- MRF-145-0011-DG-HARV-C0913/MRF_/MRF_/United Kingdom
- MC_UP_A620_1014/MRC_/Medical Research Council/United Kingdom
- MR/P020941/1/MRC_/Medical Research Council/United Kingdom
- MC_PC_21022/MRC_/Medical Research Council/United Kingdom
- MC_PC_21001/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
