

Exceeding the Limits of Static Cold Storage in Limb Transplantation Using Subnormothermic Machine Perfusion
- PMID: 35764315
- PMCID: PMC10848168
- DOI: 10.1055/a-1886-5697
Exceeding the Limits of Static Cold Storage in Limb Transplantation Using Subnormothermic Machine Perfusion
Abstract
Background: For 50 years, static cold storage (SCS) has been the gold standard for solid organ preservation in transplantation. Although logistically convenient, this preservation method presents important constraints in terms of duration and cold ischemia-induced lesions. We aimed to develop a machine perfusion (MP) protocol for recovery of vascularized composite allografts (VCA) after static cold preservation and determine its effects in a rat limb transplantation model.
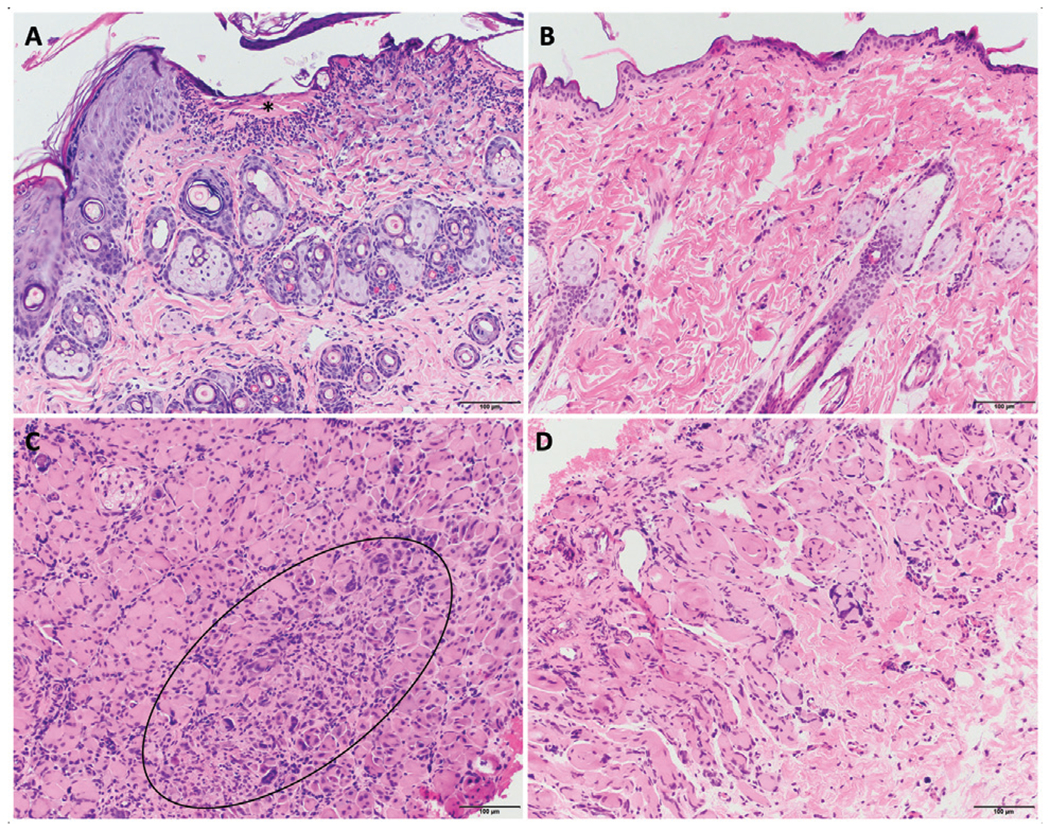
Methods: Partial hindlimbs were procured from Lewis rats and subjected to SCS in Histidine-Tryptophan-Ketoglutarate solution for 0, 12, 18, 24, and 48 hours. They were then either transplanted (Txp), subjected to subnormothermic machine perfusion (SNMP) for 3 hours with a modified Steen solution, or to SNMP + Txp. Perfusion parameters were assessed for blood gas and electrolytes measurement, and flow rate and arterial pressures were monitored continuously. Histology was assessed at the end of perfusion. For select SCS durations, graft survival and clinical outcomes after transplantation were compared between groups at 21 days.
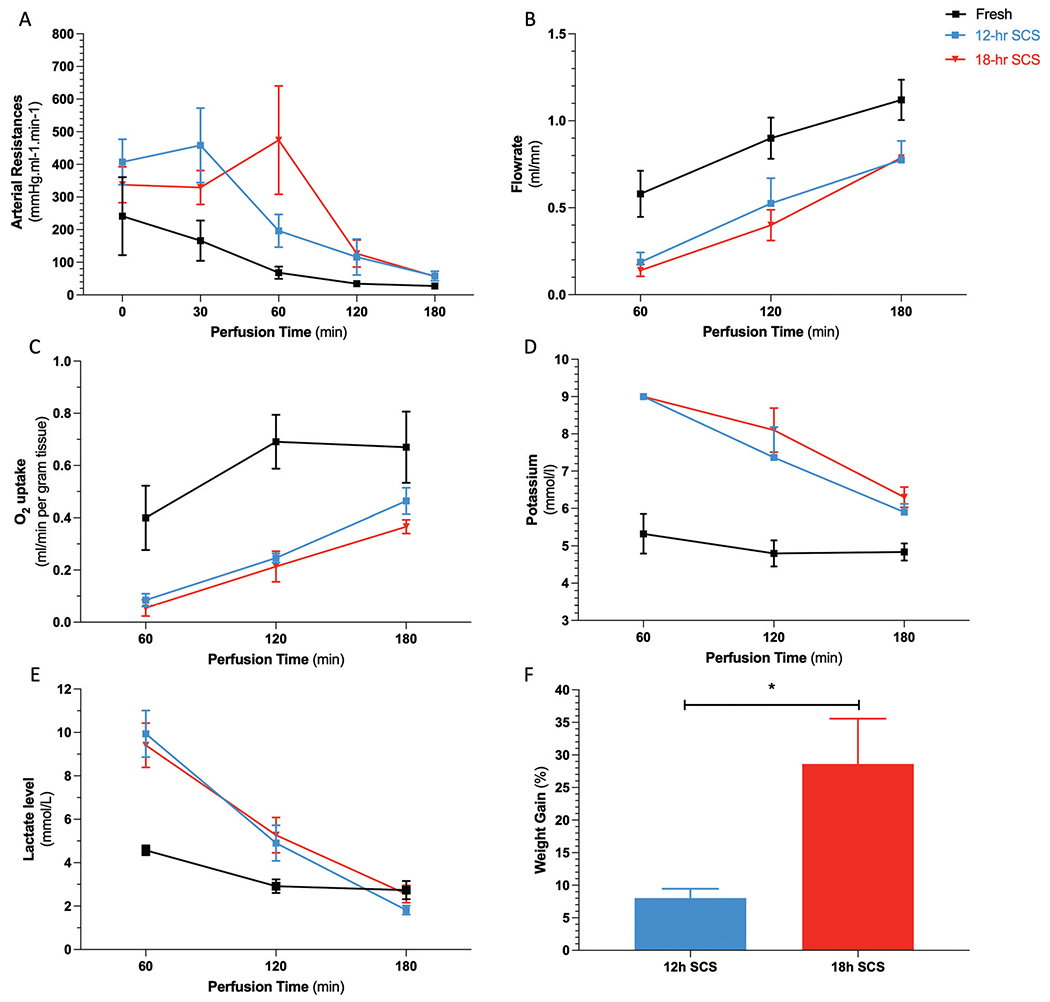
Results: Transplantation of limbs preserved for 0, 12, 18, and 24-hour SCS resulted in similar survival rates at postoperative day 21. Grafts cold-stored for 48 hours presented delayed graft failure (p = 0.0032). SNMP of limbs after 12-hour SCS recovered the vascular resistance, potassium, and lactate levels to values similar to limbs that were not subjected to SCS. However, 18-hour SCS grafts developed significant edema during SNMP recovery. Transplantation of grafts that had undergone a mixed preservation method (12-hour SCS + SNMP + Txp) resulted in better clinical outcomes based on skin clinical scores at day 21 post-transplantation when compared to the SCS + Txp group (p = 0.01613).
Conclusion: To date, VCA MP is still limited to animal models and no protocols are yet developed for graft recovery. Our study suggests that ex vivo SNMP could help increase the preservation duration and limit cold ischemia-induced injury in VCA transplantation.
Thieme. All rights reserved.
Conflict of interest statement
The authors declare competing interests. Drs. A.G.L., C.L.C., K.U., S.N.T., R.J.d.V., and C.A.P. have provisional patent applications relevant to this study. K.U. and S.N.T. have financial interests in Sylvatica Biotech Inc., a company focused on developing organ preservation technology. All competing interests are managed by Mass General Brigham in accordance with their conflict-of-interest policies.
Figures





Similar articles
-
Machine Perfusion Enables 24-h Preservation of Vascularized Composite Allografts in a Swine Model of Allotransplantation.Transpl Int. 2024 May 15;37:12338. doi: 10.3389/ti.2024.12338. eCollection 2024. Transpl Int. 2024. PMID: 38813393 Free PMC article.
-
Optimization of Ex Vivo Machine Perfusion and Transplantation of Vascularized Composite Allografts.J Surg Res. 2022 Feb;270:151-161. doi: 10.1016/j.jss.2021.09.005. Epub 2021 Oct 17. J Surg Res. 2022. PMID: 34670191 Free PMC article.
-
Determination and extension of the limits to static cold storage using subnormothermic machine perfusion.Int J Artif Organs. 2013 Nov;36(11):775-80. doi: 10.5301/ijao.5000250. Epub 2013 Oct 2. Int J Artif Organs. 2013. PMID: 24338652 Free PMC article.
-
Ex Vivo Liver Machine Perfusion: Comprehensive Review of Common Animal Models.Tissue Eng Part B Rev. 2023 Feb;29(1):10-27. doi: 10.1089/ten.TEB.2022.0018. Epub 2022 Sep 21. Tissue Eng Part B Rev. 2023. PMID: 35848526 Review.
-
Mitochondrial Consequences of Organ Preservation Techniques during Liver Transplantation.Int J Mol Sci. 2021 Mar 10;22(6):2816. doi: 10.3390/ijms22062816. Int J Mol Sci. 2021. PMID: 33802177 Free PMC article.
Cited by
-
Improving the ischemia-reperfusion injury in vascularized composite allotransplantation: Clinical experience and experimental implications.Front Immunol. 2022 Sep 16;13:998952. doi: 10.3389/fimmu.2022.998952. eCollection 2022. Front Immunol. 2022. PMID: 36189311 Free PMC article. Review.
-
Mesenchymal Stem Cell Utilization for In Vitro Donor Liver Machine Perfusion Preservation: Current Status and Future Directions.Stem Cells Transl Med. 2023 Oct 5;12(10):665-675. doi: 10.1093/stcltm/szad053. Stem Cells Transl Med. 2023. PMID: 37643740 Free PMC article. Review.
-
Study on the preservation effects of the amputated forelimb by machine perfusion at physiological temperature.Chin J Traumatol. 2024 Mar;27(2):114-120. doi: 10.1016/j.cjtee.2023.05.005. Epub 2023 May 30. Chin J Traumatol. 2024. PMID: 37311687 Free PMC article.
-
24-Hour Ex Vivo Hypothermic Acellular Perfusion of Porcine Forelimb: A 7-Day Follow-up Study.Plast Reconstr Surg. 2024 Dec 1;154(6):1138e-1148e. doi: 10.1097/PRS.0000000000011469. Epub 2024 Apr 15. Plast Reconstr Surg. 2024. PMID: 38616323 Free PMC article.
-
Machine Perfusion Enables 24-h Preservation of Vascularized Composite Allografts in a Swine Model of Allotransplantation.Transpl Int. 2024 May 15;37:12338. doi: 10.3389/ti.2024.12338. eCollection 2024. Transpl Int. 2024. PMID: 38813393 Free PMC article.
References
-
- Pribaz JJ, Caterson EJ. Evolution and limitations of conventional autologous reconstruction of the head and neck. J Craniofac Surg 2013;24(01):99–107 - PubMed
-
- Cherikh WS, Cendales LC, Wholley CL, et al. Vascularized composite allotransplantation in the United States: a descriptive analysis of the organ procurement and transplantation network data. Am J Transplant 2019;19(03):865–875 - PubMed
-
- Wainright JL, Wholley CL, Cherikh WS, Musick JM, Klassen DK. OPTN vascularized composite allograft waiting list: current status and trends in the United States. Transplantation 2018;102(11):1885–1890 - PubMed
