

Glucocorticoid therapy in respiratory illness: bench to bedside
- PMID: 35764344
- PMCID: PMC9726965
- DOI: 10.1136/jim-2021-002161
Glucocorticoid therapy in respiratory illness: bench to bedside
Abstract
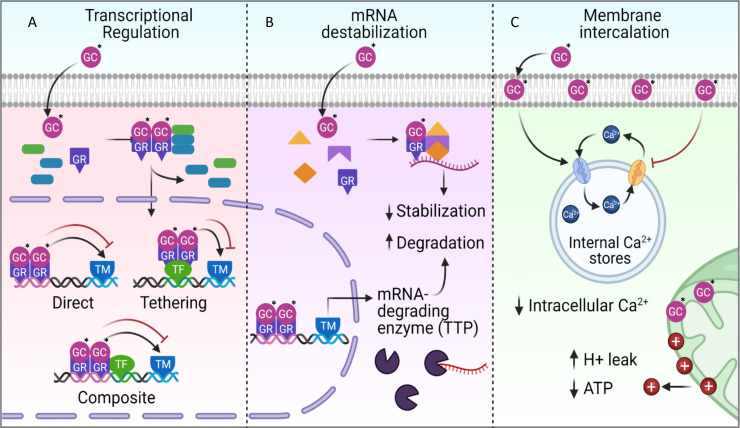
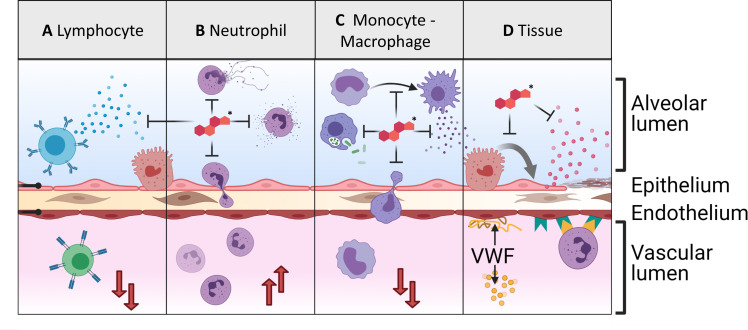
Each year, hundreds of millions of individuals are affected by respiratory disease leading to approximately 4 million deaths. Most respiratory pathologies involve substantially dysregulated immune processes that either fail to resolve the underlying process or actively exacerbate the disease. Therefore, clinicians have long considered immune-modulating corticosteroids (CSs), particularly glucocorticoids (GCs), as a critical tool for management of a wide spectrum of respiratory conditions. However, the complex interplay between effectiveness, risks and side effects can lead to different results, depending on the disease in consideration. In this comprehensive review, we present a summary of the bench and the bedside evidence regarding GC treatment in a spectrum of respiratory illnesses. We first describe here the experimental evidence of GC effects in the distal airways and/or parenchyma, both in vitro and in disease-specific animal studies, then we evaluate the recent clinical evidence regarding GC treatment in over 20 respiratory pathologies. Overall, CS remain a critical tool in the management of respiratory illness, but their benefits are dependent on the underlying pathology and should be weighed against patient-specific risks.
Keywords: anti-inflammatory agents; critical care; glucocorticoids; lung diseases; respiratory system.
© American Federation for Medical Research 2022. Re-use permitted under CC BY-NC. No commercial re-use. Published by BMJ.
Conflict of interest statement
Competing interests: Octavian Ioachimescu is an Associate Editor for the Journal of Investigative Medicine.
Figures
References
-
- Cruz-Topete D, Cidlowski JA. Glucocorticoids: Molecular Mechanisms of Action. In: Riccardi C, Levi-Schaffer F, Tiligada E, eds. Immunopharmacology and inflammation. Cham: Springer International Publishing, 2018: 249–66.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
