

Environmental variables and genome-environment interactions predicting IBD diagnosis in large UK cohort
- PMID: 35764673
- PMCID: PMC9240024
- DOI: 10.1038/s41598-022-13222-0
Environmental variables and genome-environment interactions predicting IBD diagnosis in large UK cohort
Abstract
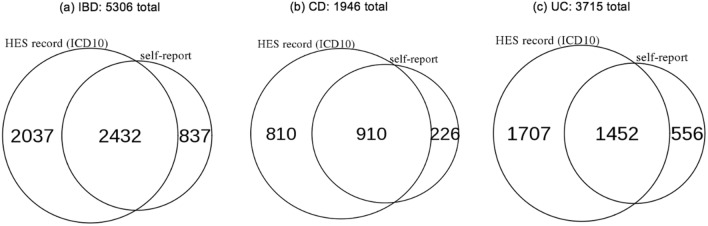
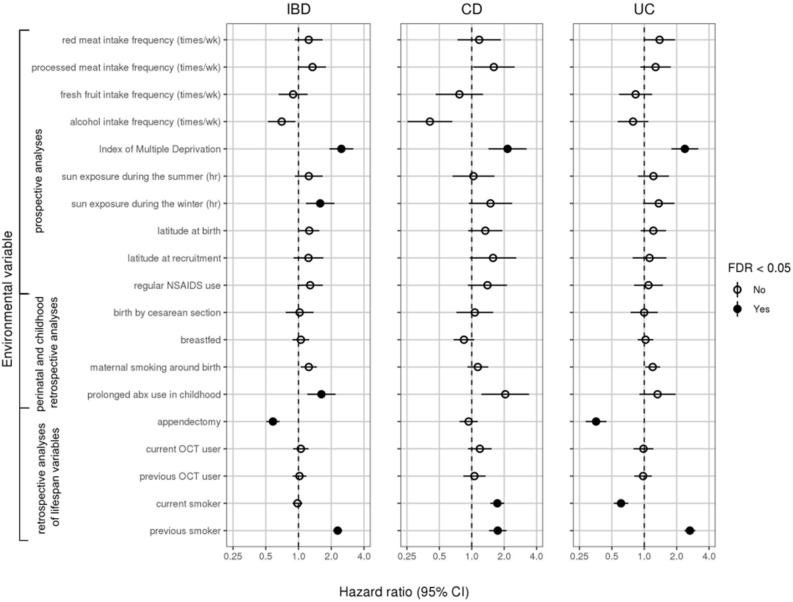
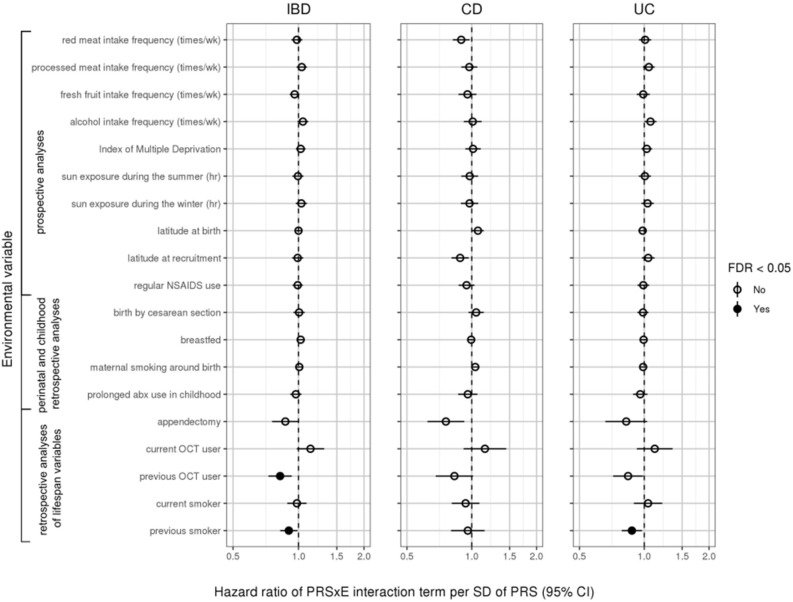
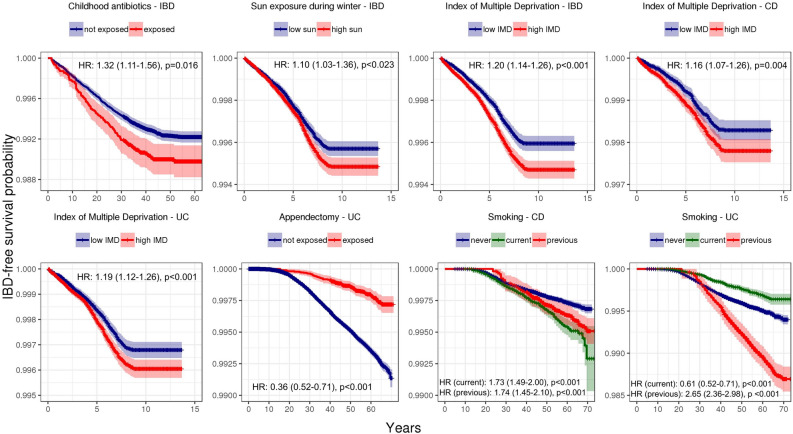
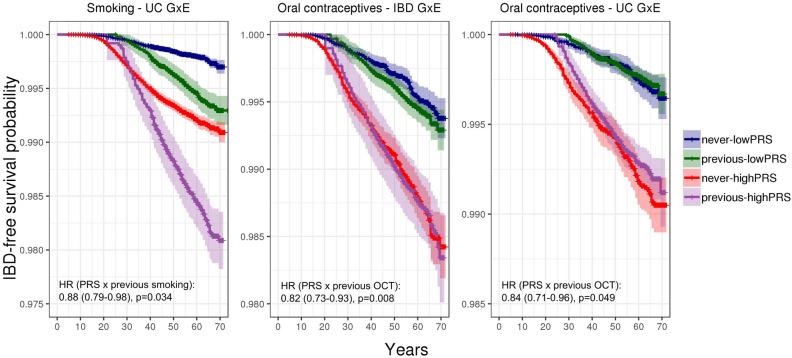
A combination of genetic susceptibility and environmental exposure is thought to cause inflammatory bowel disease (IBD), but the non-genetic component remains poorly characterized. We therefore undertook a search for environmental variables and gene-environment interactions associated with future IBD diagnosis in a large UK cohort. Using self-report and electronic health records, we identified 1946 Crohn's disease (CD) and 3715 ulcerative colitis (UC) patients after quality control in the UK Biobank. Based on prior literature and biological plausibility , we tested 38 candidate environmental variables for association with CD, UC, and overall IBD using Cox proportional hazard regressions. We also tested whether these variables interacted with polygenic risk in predicting disease, following up significant (FDR < 0.05) results with tests for SNP-environment associations. We performed robustness analyses on all significant results. As in previous reports, appendectomy protected against UC, smoking (both current and previous) elevated risk for CD, current smoking protected against UC, and previous smoking imparted a risk for UC. Childhood antibiotic use associated with IBD, as did sun exposure during the winter. Socioeconomic deprivation was conferred a risk for IBD, CD, and UC. We uncovered negative interactions between polygenic risk and previous oral contraceptive use for IBD and UC. Polygenic risk also interacted negatively with previous smoking in predicting UC. There were no individually significant SNP-environment interactions. Thus, for a limited set of environmental variables, there was strong evidence of association with IBD diagnosis in the UK Biobank, and interaction with polygenic risk was minimal.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Ng SC, Shi HY, Hamidi N, Underwood FE, Tang W, Benchimol EI, Panaccione R, Ghosh S, Wu JCY, Chan FKL, Sung JJY, Kaplan GG. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: A systematic review of population-based studies. Lancet (London, England) 2018;390(10114):2769–2778. - PubMed
-
- Liu JZ, van Sommeren S, Huang H, Ng SC, Alberts R, Takahashi A, Ripke S, Lee JC, Jostins L, Shah T, Abedian S, Cheon JH, Cho J, Dayani NE, Franke L, Fuyuno Y, Hart A, Juyal RC, Juyal G, Kim WH, Morris AP, Poustchi H, Newman WG, Midha V, Orchard TR, Vahedi H, Sood A, Sung JY, Malekzadeh R, Westra H-J, Yamazaki K, Yang S-K, International Multiple Sclerosis Genetics Consortium, International IBD Genetics Consortium. Barrett JC, Alizadeh BZ, Parkes M, Bk T, Daly MJ, Kubo M, Anderson CA, Weersma RK. Association analyses identify 38 susceptibility loci for inflammatory bowel disease and highlight shared genetic risk across populations. Nat. Genet. 2015;47(9):979–986. - PMC - PubMed
-
- de Lange KM, Moutsianas L, Lee JC, Lamb CA, Luo Y, Kennedy NA, Jostins L, Rice DL, Gutierrez-Achury J, Ji S-G, Heap G, Nimmo ER, Edwards C, Henderson P, Mowat C, Sanderson J, Satsangi J, Simmons A, Wilson DC, Tremelling M, Hart A, Mathew CG, Newman WG, Parkes M, Lees CW, Uhlig H, Hawkey C, Prescott NJ, Ahmad T, Mansfield JC, Anderson CA, Barrett JC. Genome-wide association study implicates immune activation of multiple integrin genes in inflammatory bowel disease. Nat. Genet. 2017;49(2):256–261. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
