

Household food insecurity, sense of community belonging, and access to a regular medical doctor as mediators in the relationship between mood and/or anxiety disorders and self-rated general health in Canada between 2011 and 2016: a serial cross-sectional analysis
- PMID: 35764860
- PMCID: PMC9663790
- DOI: 10.17269/s41997-022-00658-0
Household food insecurity, sense of community belonging, and access to a regular medical doctor as mediators in the relationship between mood and/or anxiety disorders and self-rated general health in Canada between 2011 and 2016: a serial cross-sectional analysis
Abstract
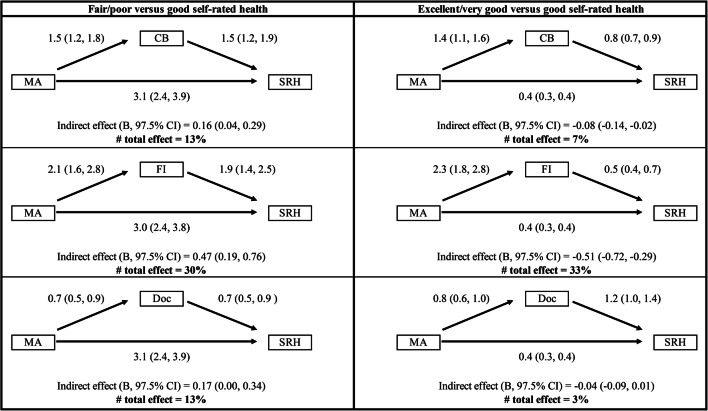
Objective: To assess whether (household) food insecurity, access to a regular medical doctor, and sense of community belonging mediate the relationship between mood and/or anxiety disorders and self-rated general health.
Methods: We used six annual cycles of the Canadian Community Health Survey, including Canadian adults aged 18-59 years, between 2011 and 2016. Mediation models, adjusted for key determinants of health, were based on a series of weighted logistic regression models. The Sobel products of coefficients approach was used to estimate the indirect effect, and bootstrapping to estimate uncertainty.
Results: The annual (weighted) prevalence of mood and/or anxiety disorders increased from 11.3% (2011) to 13.2% (2016). Across the 6 years, 23.9-27.7% of individuals with mood and/or anxiety disorders reported fair/poor self-rated health as compared with 4.9-6.5% of those without mood and/or anxiety disorders (p<0.001). Similarly, the 7.2-8.9% of the population reporting fair/poor self-rated health were disproportionately represented among individuals reporting food insecurity (21.1-26.2%, p<0.001) and a weak sense of community belonging (10.0-12.2%, p<0.001). A significantly lower prevalence of poor self-rated health was observed among respondents reporting having access to a regular medical doctor in 2012, 2015, and 2016. In 2016, sense of community belonging and food insecurity significantly mediated the effect of mood and/or anxiety disorders on self-rated general health. Access to a regular medical doctor did not mediate this relationship.
Conclusion: Efficient policies that address food insecurity and sense of community belonging are needed to decrease the mental health burden and improve health satisfaction of Canadians.
RéSUMé: OBJECTIF: Déterminer si l’insécurité alimentaire (du ménage), l’accès à un médecin traitant et le sentiment d’appartenance à la communauté modèrent le lien entre les troubles anxieux et/ou de l’humeur et la santé générale autoévaluée. MéTHODE: Nous avons utilisé six cycles annuels (2011 à 2016) de l’Enquête sur la santé dans les collectivités canadiennes incluant des Canadiens adultes de 18 à 59 ans. Nos modèles de modération, ajustés selon les principaux déterminants de la santé, reposaient sur une série de modèles de régression logistique pondérés. Nous avons utilisé l’approche des produits des coefficients de Sobel pour estimer les effets indirects, et l’autoamorçage pour estimer l’incertitude. RéSULTATS: La prévalence annuelle (pondérée) des troubles anxieux et/ou de l’humeur a augmenté, passant de 11,3 % en 2011 à 13,2 % en 2016. Sur la période de six ans, 23,9 à 27,7 % des personnes ayant des troubles anxieux et/ou de l’humeur ont déclaré avoir une santé moyenne/mauvaise, contre 4,9 à 6,5 % des personnes n’ayant pas de troubles anxieux et/ou de l’humeur (p < 0,001). De même, les 7,2 à 8,9 % de la population ayant déclaré avoir une santé moyenne/mauvaise étaient disproportionnellement représentés chez les personnes disant être en situation d’insécurité alimentaire (21,1-26,2 %, p < 0,001) et avoir un faible sentiment d’appartenance à la communauté (10,0-12,2 %, p < 0,001). Une prévalence significativement plus faible de mauvaise santé autoévaluée a été observée chez les répondants ayant dit avoir accès à un médecin traitant en 2012, 2015 et 2016. En 2016, le sentiment d’appartenance à la communauté et l’insécurité alimentaire modéraient de façon significative l’effet des troubles anxieux et/ou de l’humeur sur la santé générale autoévaluée. L’accès à un médecin traitant ne modérait pas ce lien. CONCLUSION: Des politiques efficaces pour aborder l’insécurité alimentaire et le sentiment d’appartenance à la communauté sont nécessaires pour réduire le fardeau des troubles mentaux et améliorer la satisfaction des Canadiens face à leur santé.
Keywords: Anxiety; Community connectedness; Healthcare access; Household food insecurity; Mental health; Mood disorder; Self-rated general health; Sense of community belonging.
© 2022. The Author(s) under exclusive license to The Canadian Public Health Association.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Food insecurity and mental health during the COVID-19 pandemic.Health Rep. 2020 Dec 16;31(12):3-11. doi: 10.25318/82-003-x202001200001-eng. Health Rep. 2020. PMID: 33325672
-
Life stress as a mediator and community belonging as a moderator of mood and anxiety disorders and co-occurring disorders with heavy drinking of gay, lesbian, bisexual, and heterosexual Canadians.Soc Psychiatry Psychiatr Epidemiol. 2016 Aug;51(8):1181-92. doi: 10.1007/s00127-016-1236-1. Epub 2016 May 13. Soc Psychiatry Psychiatr Epidemiol. 2016. PMID: 27178431
-
Food insecurity is associated with mental health problems among Canadian youth.J Epidemiol Community Health. 2021 Aug;75(8):741-748. doi: 10.1136/jech-2020-216149. Epub 2021 Feb 12. J Epidemiol Community Health. 2021. PMID: 33579754
-
Household Food Insecurity Narrows the Sex Gap in Five Adverse Mental Health Outcomes among Canadian Adults.Int J Environ Res Public Health. 2019 Jan 24;16(3):319. doi: 10.3390/ijerph16030319. Int J Environ Res Public Health. 2019. PMID: 30678378 Free PMC article.
-
A Systematic Review and Meta-analysis of Depression, Anxiety, and Sleep Disorders in US Adults with Food Insecurity.J Gen Intern Med. 2019 Dec;34(12):2874-2882. doi: 10.1007/s11606-019-05202-4. Epub 2019 Aug 5. J Gen Intern Med. 2019. PMID: 31385212 Free PMC article.
Cited by
-
Prevalence and characteristics of healthcare utilization with different providers among Canadians with chronic back problems: A population-based study.Brain Spine. 2024 Apr 16;4:102812. doi: 10.1016/j.bas.2024.102812. eCollection 2024. Brain Spine. 2024. PMID: 38698804 Free PMC article.
-
The influence of alcohol consumption on Self-Rated Health and Mood during the COVID-19 pandemic in Spain.Front Public Health. 2023 Oct 10;11:1257459. doi: 10.3389/fpubh.2023.1257459. eCollection 2023. Front Public Health. 2023. PMID: 37886053 Free PMC article.
-
The relationship between Sense of Community and perceived service quality: rethinking the role of local communities in sustaining rural health and social care.BMC Health Serv Res. 2025 May 19;25(1):716. doi: 10.1186/s12913-025-12817-3. BMC Health Serv Res. 2025. PMID: 40389999 Free PMC article.
-
Sense of Community in the context of disease prevention and health promotion: A scoping review of the literature.BMC Public Health. 2024 Nov 8;24(1):3090. doi: 10.1186/s12889-024-20515-8. BMC Public Health. 2024. PMID: 39516795 Free PMC article.
References
-
- Bassett E, Moore S. Mental health and social capital: Social capital as a promising initiative to improving the mental health of communities (Chapter 28) 2013.
-
- Canadian Medical Association. (2018). Ensuring equitable access to health care: Strategies for governments, health system planners, and the medical profession. Retrieved 20 January 2020 from https://policybase.cma.ca/en/permalink/policy11062
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
