

The Collaborative Ocular Tuberculosis Study (COTS) calculator-a consensus-based decision tool for initiating antitubercular therapy in ocular tuberculosis
- PMID: 35764876
- PMCID: PMC10170101
- DOI: 10.1038/s41433-022-02147-7
The Collaborative Ocular Tuberculosis Study (COTS) calculator-a consensus-based decision tool for initiating antitubercular therapy in ocular tuberculosis
Abstract
Objective: To introduce the Collaborative Ocular Tuberculosis Study (COTS) Calculator, an online clinical scoring system for initiating antitubercular therapy (ATT) in patients with ocular tuberculosis (TB).
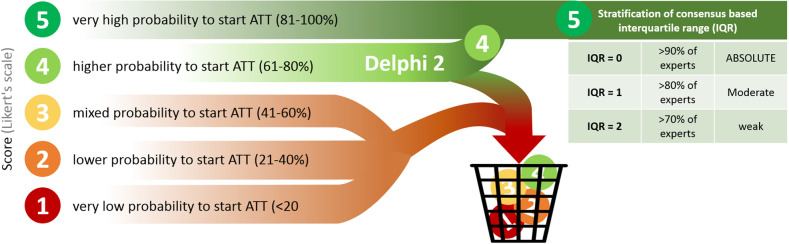
Method: The COTS Calculator was derived from COTS Consensus (COTS CON) data, which has previously published consensus guidelines. Using a two-step Delphi method, 81 experts evaluated 486 clinical scenario-based questions, ranking their likelihood of initiating ATT in each specific scenario. Each scenario was a permutation of the results and/or availability of five following components-clinical phenotype, endemicity, two immunological (tuberculin skin test, interferon-γ release assay) and one radiological (chest X-Ray) test results-and a sixth component further stratifying three of the clinical phenotypes. The median scores and interquartile ranges (IQR) of each scenario were tabulated, representing the expert consensus on whether to initiate ATT in that scenario. The consensus table was encoded to develop the COTS Calculator.
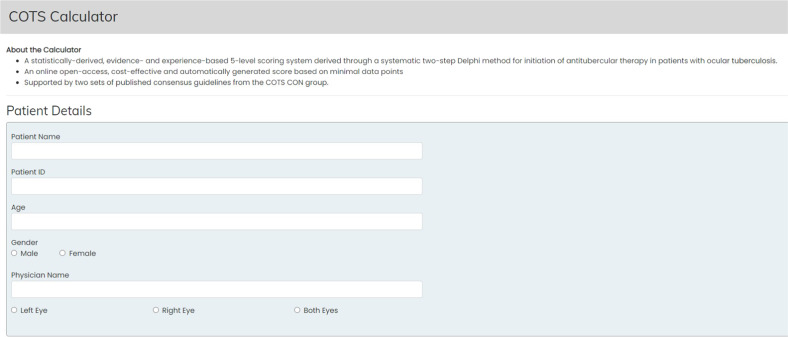
Results: The COTS Calculator can be accessed online at: https://www.oculartb.net/cots-calc . The attending physician can select the conditions present in the patient, which will generate a median score from 1 to 5. 114 out of 486 scenarios (24%) deliberated had a median score of 5 indicating expert consensus to initiate ATT.
Conclusion: The COTS Calculator is an efficient, low-cost, evidence and experience-based clinical tool to guide ATT initiation. While it holds substantial promise in improving standard-of-care for ocular-TB patients, future validation studies can help to as certain its clinical utility and reliability.
© 2022. The Author(s), under exclusive licence to The Royal College of Ophthalmologists.
Conflict of interest statement
RA, ZL, BB, IT, SM, AR, JHK, JRS, PM, QDN, CP and VG report no competing interests, financial or propriety, in the subject matter or materials discussed in this paper. JHK is a consultant for Gilead Pharma, a company evaluating a treatment for non-infectious uveitis, and equity owner for Betaliq, a company developing an intraocular pressure-lowering treatment. RA is supported by a grant from the National Medical Research Council (NMRC) by Ministry of Health, Singapore, for the Clinician Scientist Award (CSA) from 2020 to 2023. He has not received funding for his work in this publication.
Figures


Similar articles
-
Validation of the Online Collaborative Ocular Tuberculosis Study Calculator for Tubercular Uveitis.JAMA Ophthalmol. 2024 Dec 1;142(12):1140-1148. doi: 10.1001/jamaophthalmol.2024.4567. JAMA Ophthalmol. 2024. PMID: 39480402
-
Collaborative Ocular Tuberculosis Study Consensus Guidelines on the Management of Tubercular Uveitis-Report 2: Guidelines for Initiating Antitubercular Therapy in Anterior Uveitis, Intermediate Uveitis, Panuveitis, and Retinal Vasculitis.Ophthalmology. 2021 Feb;128(2):277-287. doi: 10.1016/j.ophtha.2020.06.052. Epub 2020 Jun 27. Ophthalmology. 2021. PMID: 32603726
-
Collaborative Ocular Tuberculosis Study Consensus Guidelines on the Management of Tubercular Uveitis-Report 1: Guidelines for Initiating Antitubercular Therapy in Tubercular Choroiditis.Ophthalmology. 2021 Feb;128(2):266-276. doi: 10.1016/j.ophtha.2020.01.008. Epub 2020 Jan 11. Ophthalmology. 2021. PMID: 32115264
-
The Collaborative Ocular Tuberculosis Study (COTS) Consensus (CON) Group Meeting Proceedings.Ocul Immunol Inflamm. 2020 Sep 30;28(sup1):85-95. doi: 10.1080/09273948.2020.1716025. Epub 2020 Apr 6. Ocul Immunol Inflamm. 2020. PMID: 32250731
-
Ocular tuberculosis: Where are we today?Indian J Ophthalmol. 2020 Sep;68(9):1808-1817. doi: 10.4103/ijo.IJO_1451_20. Indian J Ophthalmol. 2020. PMID: 32823397 Free PMC article. Review.
Cited by
-
Advanced drug delivery and therapeutic strategies for tuberculosis treatment.J Nanobiotechnology. 2023 Nov 9;21(1):414. doi: 10.1186/s12951-023-02156-y. J Nanobiotechnology. 2023. PMID: 37946240 Free PMC article. Review.
-
Infectious eye disease in the 21st century-an overview.Eye (Lond). 2024 Aug;38(11):2014-2027. doi: 10.1038/s41433-024-02966-w. Epub 2024 Feb 14. Eye (Lond). 2024. PMID: 38355671 Free PMC article. Review.
-
Diagnosis and biomarkers for ocular tuberculosis: From the present into the future.Theranostics. 2023 Apr 1;13(7):2088-2113. doi: 10.7150/thno.81488. eCollection 2023. Theranostics. 2023. PMID: 37153734 Free PMC article. Review.
-
Rare bilateral corneoscleral perforation secondary to ocular tuberculosis: a case report and clinical insights.J Ophthalmic Inflamm Infect. 2025 Mar 5;15(1):16. doi: 10.1186/s12348-025-00472-y. J Ophthalmic Inflamm Infect. 2025. PMID: 40038144 Free PMC article.
-
Validation of the Online Collaborative Ocular Tuberculosis Study Calculator for Tubercular Uveitis.JAMA Ophthalmol. 2024 Dec 1;142(12):1140-1148. doi: 10.1001/jamaophthalmol.2024.4567. JAMA Ophthalmol. 2024. PMID: 39480402
References
-
- World Health Organization. Global Tuberculosis Report. 2021. https://www.who.int/publications/i/item/9789240037021.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
