

Impact of the COVID-19 pandemic on delays in surgical procedures in Germany: a multi-center analysis of an administrative registry of 176,783 patients
- PMID: 35765000
- PMCID: PMC9238103
- DOI: 10.1186/s13037-022-00331-y
Impact of the COVID-19 pandemic on delays in surgical procedures in Germany: a multi-center analysis of an administrative registry of 176,783 patients
Abstract
Background: While extensive data are available on the postponement of elective surgical procedures due to the COVID-19 pandemic for Germany, data on the impact on emergency procedures is limited.
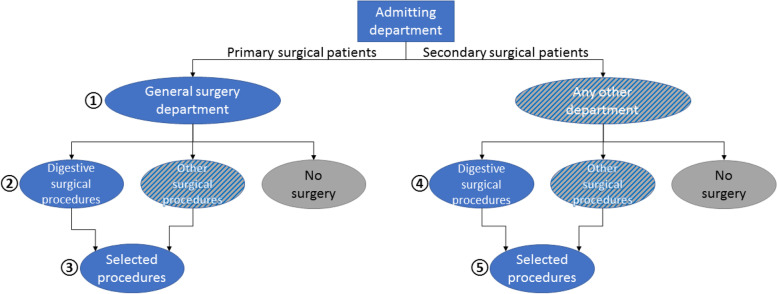
Methods: In this retrospective case-control study, anonymized case-related routine data of a Germany-wide voluntary hospital association (CLINOTEL association) of 66 hospitals was analyzed. Operation volumes, in-hospital mortality, and COVID-19 prevalence rates in digestive surgery procedure groups and selected single surgical procedures in the one-year periods before and after the outbreak of the COVID-19 pandemic were analyzed. The analysis was stratified by admitting department (direct admission or transfer to the general surgical department, i.e., primary or secondary surgical patients) and type of admission (elective/emergent).
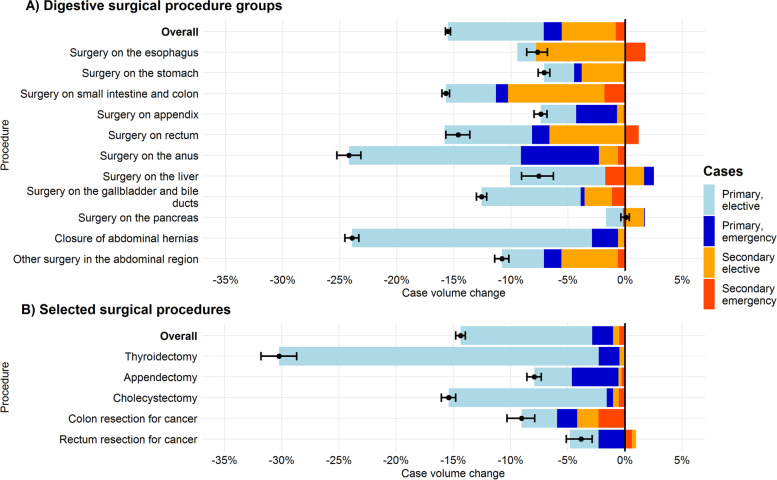
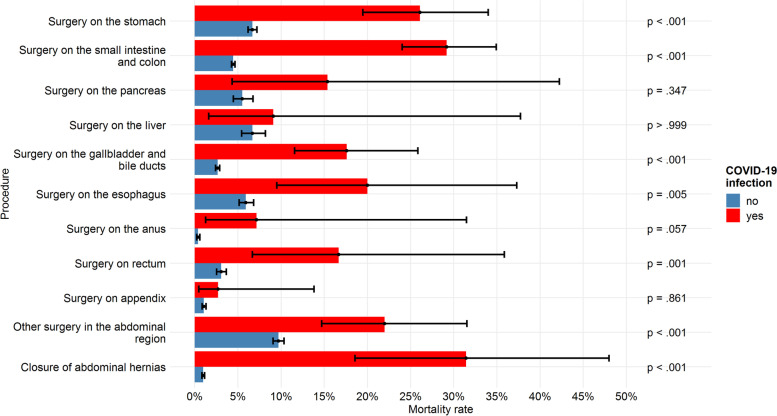
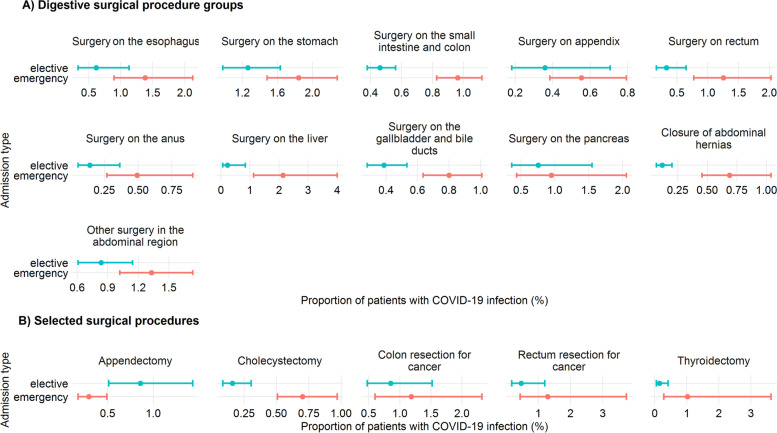
Results: The total number of primary and secondary surgical patients decreased by 22.7% and 11.7%, respectively. Among primary surgical patients more pronounced reductions were observed in elective (-25.6%) than emergency cases (-18.8%). Most affected procedures were thyroidectomies (-30.2%), operations on the anus (-24.2%), and closure of abdominal hernias (-23.9%; all P's < 0.001). Declines were also observed in colorectal (-9.0%, P = 0.002), but not in rectal cancer surgery (-3.9%, n.s.). Mortality was slightly increased in primary (1.3 vs. 1.5%, P < 0.001), but not in secondary surgical cases. The one-year prevalence of COVID-19 in general surgical patients was low (0.6%), but a significant driver of mortality (OR = 9.63, P < 0.001).
Conclusions: Compared to the previous year period, the number of patients in general and visceral surgery decreased by 22.7% in the first pandemic year. At the procedure level, a decrease of 14.8% was observed for elective procedures and 6.0% for emergency procedures. COVID-19 infections in general surgical patients are rare (0.6% prevalence), but associated with high mortality (21.8%).
Trial registration: The present study does not meet the ICMJE definition of a clinical trial and was therefore not registered.
Keywords: COVID-19; Elective surgery; Emergent surgery; General surgery; Health care research.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Belkacemi Y, Grellier N, Ghith S, et al. A review of the international early recommendations for departments organization and cancer management priorities during the global COVID-19 pandemic: applicability in low- and middle-income countries. Eur J Cancer. 2020;135:130–146. doi: 10.1016/j.ejca.2020.05.015. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
