

Patient-reported outcomes in a Chinese cohort of osteogenesis imperfecta unveil psycho-physical stratifications associated with clinical manifestations
- PMID: 35765008
- PMCID: PMC9238011
- DOI: 10.1186/s13023-022-02394-7
Patient-reported outcomes in a Chinese cohort of osteogenesis imperfecta unveil psycho-physical stratifications associated with clinical manifestations
Abstract
Background: Osteogenesis imperfecta (OI) is a rare congenital disorder of the skeletal system, inflicting debilitating physical and psychological distress on patients and caregivers. Over the decades, much effort has been channeled towards understanding molecular mechanisms and developing new treatments. It has recently become more apparent that patient-reported outcome measurements (PROM) during treatment, healing and rehabilitation are helpful in facilitating smoother communication, refining intervention strategies and achieving higher quality of life. To date, systematic analyses of PROM in OI patients remain scarce.
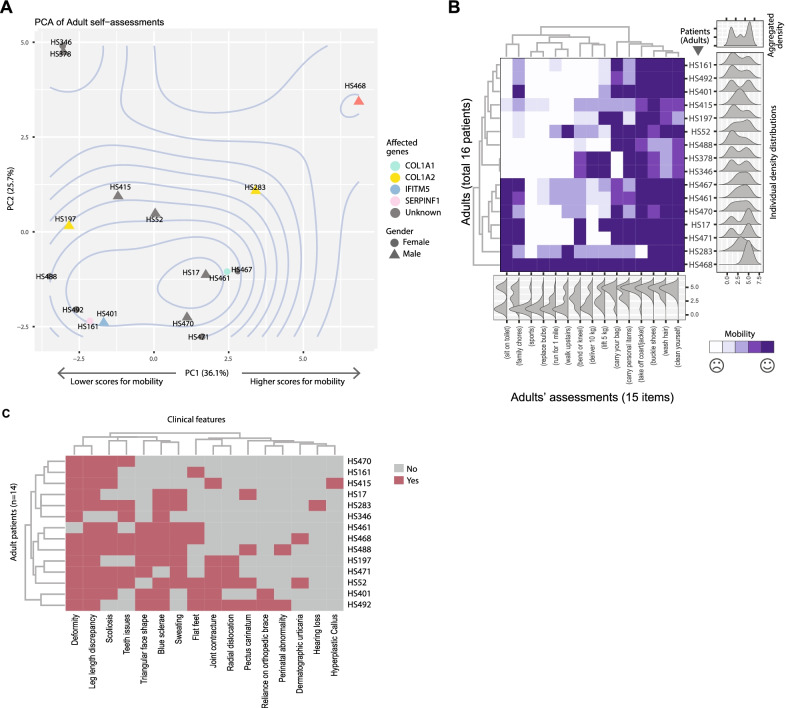
Results: Here, utilizing a PROM Information System, we report a cross-sectional and longitudinal study in a southern Chinese cohort of 90 OI patients, covering both the child and adult age-groups. In the child group where both self and parental surveys were obtained, we identified two clusters of comparable sizes showing different outlooks in physical mobility and emotional experiences. One cluster (Cluster 1) is more negative about themselves than the other (Cluster 2). A concordance of 84.7% between self and parental assessments was recorded, suggesting the stability and validity of PROM-based stratification. Clinical subtyping, deformity, leg length discrepancy, and limited joint mobility were significantly associated with this stratification, with Cluster 1 showing higher percentages of severe phenotypes than Cluster 2. Since OI is a genetic disorder, we performed genetic testing on 72 of the 90 patients, but found no obvious association between genotypes and the PROM stratification. Analyses of longitudinal data suggested that patients tended to stay in the same psychological state, in both clusters. Adult patients also showed a continuous spectrum of self-evaluation that matches their clinical manifestations.
Conclusion: By systematically analyzing patient-reported outcomes, our study demonstrated the link between the sociopsychological wellbeing of OI patients, and their clinical manifestations, which may serve as the basis for evaluating clinical interventions and help achieve better patient-centric medical practices. The lack of genotype-PROM association may be due to the diverse mutational spectrum in OI, which warrants further investigation when a larger sample size is available.
Keywords: Adults; Children; Cross-sectional; Genetic testing; Longitudinal; Osteogenesis imperfecta; PROM; Patient stratification; Psycho-physical; Rare disease.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures






References
-
- Marini JC, Forlino A, Cabral WA, Barnes AM, San Antonio JD, Milgrom S, et al. Consortium for osteogenesis imperfecta mutations in the helical domain of type I collagen: regions rich in lethal mutations align with collagen binding sites for integrins and proteoglycans. Hum Mutat. 2007;28(3):209–221. doi: 10.1002/humu.20429. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
