

A nomogram to predict the in-hospital mortality of patients with congestive heart failure and chronic kidney disease
- PMID: 35765720
- PMCID: PMC9715887
- DOI: 10.1002/ehf2.14042
A nomogram to predict the in-hospital mortality of patients with congestive heart failure and chronic kidney disease
Abstract
Aims: Patients with congestive heart failure (CHF) may also suffer from chronic kidney disease (CKD), and the two conditions may interact to increase the risk of death. The purpose of this study was to investigate the risk factors contributing to in-hospital mortality in patients with CHF and CKD and to develop a nomogram to predict the risk of in-hospital mortality.
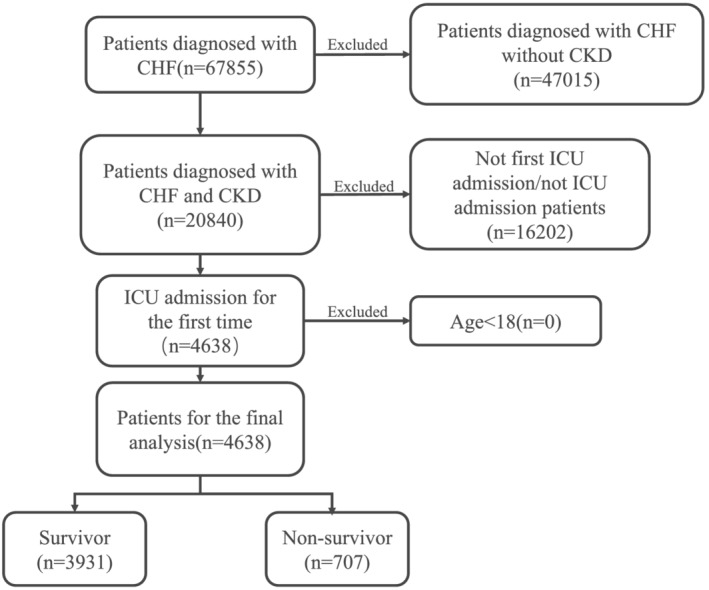
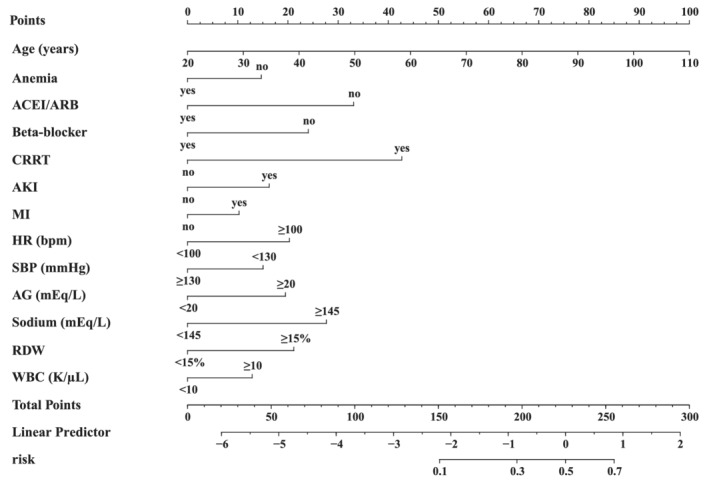
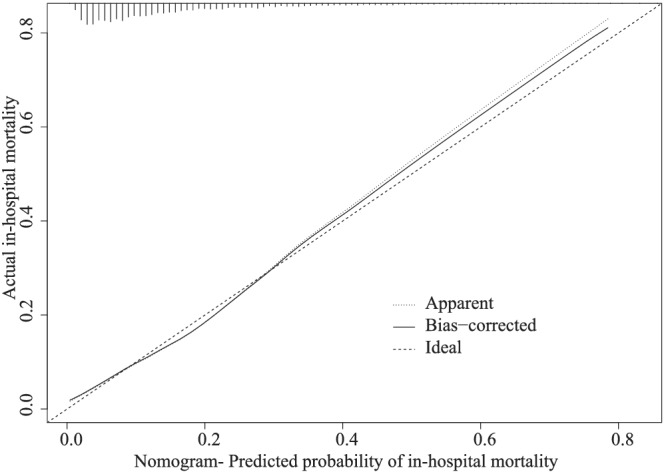
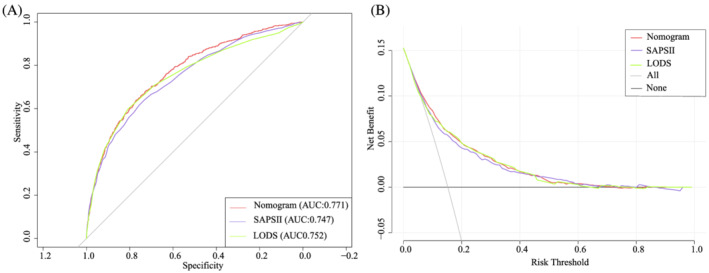
Methods and results: This retrospective study used data from the Marketplace for Medical Information in Intensive Care (MIMIC-IV, version 1.0). Patients diagnosed with CHF and CKD in MIMIC-IV were included in this study. The least absolute shrinkage and selection operator (LASSO) logistic regression is used to select risk variables for the nomogram model, and bootstrap is used for internal validation. Simplified Acute Physiology Score II (SAPS II) and Logistic Organ Dysfunction Score (LODS) were compared with the nomogram model by the area under the receiver operating characteristic curve (AUC) and decision curve analysis (DCA). A total of 4638 adult patients with CHF and CKD were included in the final cohort; of them, 707 (15.2%) died and 3931 (84.8%) survived during hospitalization. Our final model included the following 13 variables: age, acute kidney injury, myocardial infarction, anaemia, heart rate ≥ 100 b.p.m., systolic blood pressure ≥ 130 mmHg, anion gap (AG) ≥ 20 mEq/L, sodium ≥ 145 mEq/L, red blood cell distribution width (RDW) ≥ 15.5%, white blood cell count ≥ 10 K/μL, continuous renal replacement therapy (CRRT), angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, and beta-blocker. The corrected C-statistic of the nomogram was 0.767, and the calibration curve indicating good concordance between the predicted and observed values. The nomogram demonstrated good accuracy for predicting the in-hospital mortality with an AUC of 0.771 (95% CI: 0.752-0.790), while the AUC for SAPS II and LODS was 0.747 (95% CI: 0.726-0.767) and 0.752 (95% CI: 0.730-0.773), respectively. DCA found that when the threshold probability was 0.05 to 0.41, the nomogram model could provide a greater net benefit than SAPS II.
Conclusions: In this retrospective cohort analysis of patients with CHF and CKD, we identified 13 independent variables associated with in-hospital mortality using LASSO logistic regression. RDW, AG, and CRRT were reported to play a significant role in in-hospital mortality among patients with CHF and CKD for the first time. Based on a simplified model including 13 variables, a nomogram was drawn to predict the risk of in-hospital mortality. In comparison with SAPS II and LODS, the nomogram model performed well.
Keywords: Anion gap; Chronic kidney disease; Congestive heart failure; Continuous renal replacement therapy; MIMIC-IV; Nomogram; Red blood cell distribution width.
© 2022 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
None declared.
Figures
Similar articles
-
[Establishment and evaluation of early in-hospital death prediction model for patients with acute pancreatitis in intensive care unit].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023 Aug;35(8):865-869. doi: 10.3760/cma.j.cn121430-20220713-00660. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023. PMID: 37593868 Chinese.
-
A nomogram for predicting short-term mortality in ICU patients with coexisting chronic obstructive pulmonary disease and congestive heart failure.Respir Med. 2024 Nov-Dec;234:107803. doi: 10.1016/j.rmed.2024.107803. Epub 2024 Sep 7. Respir Med. 2024. PMID: 39251097
-
A new nomogram to predict in-hospital mortality in patients with acute decompensated chronic heart failure and diabetes after 48 Hours of Intensive Care Unit.BMC Cardiovasc Disord. 2024 Apr 6;24(1):199. doi: 10.1186/s12872-024-03848-5. BMC Cardiovasc Disord. 2024. PMID: 38582861 Free PMC article.
-
A nomogram for predicting the 4-year risk of chronic kidney disease among Chinese elderly adults.Int Urol Nephrol. 2023 Jun;55(6):1609-1617. doi: 10.1007/s11255-023-03470-y. Epub 2023 Jan 31. Int Urol Nephrol. 2023. PMID: 36720744 Review.
-
Statistical Methods for Recurrent Event Analysis in Cohort Studies of CKD.Clin J Am Soc Nephrol. 2017 Dec 7;12(12):2066-2073. doi: 10.2215/CJN.12841216. Epub 2017 Jul 17. Clin J Am Soc Nephrol. 2017. PMID: 28716856 Free PMC article. Review.
Cited by
-
Prognostic value of anion gap for patients with heart failure: a systematic review and meta-analysis.BMC Cardiovasc Disord. 2024 Dec 20;24(1):727. doi: 10.1186/s12872-024-04420-x. BMC Cardiovasc Disord. 2024. PMID: 39707227 Free PMC article.
-
[Prediction of risk of in-hospital death in patients with chronic heart failure complicated by lung infections using interpretable machine learning].Nan Fang Yi Ke Da Xue Xue Bao. 2024 Jun 20;44(6):1141-1148. doi: 10.12122/j.issn.1673-4254.2024.06.15. Nan Fang Yi Ke Da Xue Xue Bao. 2024. PMID: 38977344 Free PMC article. Chinese.
-
Predicting 28-day all-cause mortality in patients admitted to intensive care units with pre-existing chronic heart failure using the stress hyperglycemia ratio: a machine learning-driven retrospective cohort analysis.Cardiovasc Diabetol. 2025 Jan 8;24(1):10. doi: 10.1186/s12933-025-02577-z. Cardiovasc Diabetol. 2025. PMID: 39780223 Free PMC article.
-
Associations of continuous anionic gap detection with the mortality in critically ill patients receiving renal replacement therapy.Int Urol Nephrol. 2023 Nov;55(11):2967-2980. doi: 10.1007/s11255-023-03583-4. Epub 2023 Apr 7. Int Urol Nephrol. 2023. PMID: 37027077 Free PMC article.
-
Development and validation of a prediction model for in-hospital death in patients with heart failure and atrial fibrillation.BMC Cardiovasc Disord. 2023 Oct 11;23(1):505. doi: 10.1186/s12872-023-03521-3. BMC Cardiovasc Disord. 2023. PMID: 37821809 Free PMC article.
References
-
- Maggioni AP, Dahlstrom U, Filippatos G, Chioncel O, Crespo Leiro M, Drozdz J, Fruhwald F, Gullestad L, Logeart D, Fabbri G, Urso R, Metra M, Parissis J, Persson H, Ponikowski P, Rauchhaus M, Voors AA, Nielsen OW, Zannad F, Tavazzi L, Heart Failure Association of the European Society of Cardiology (HFA) . Eurobservational research programme: Regional differences and 1‐year follow‐up results of the heart failure pilot survey (esc‐hf pilot). Eur J Heart Fail. 2013; 15: 808–817. - PubMed
-
- Schefold JC, Filippatos G, Hasenfuss G, Anker SD, von Haehling S. Heart failure and kidney dysfunction: Epidemiology, mechanisms and management. Nat Rev Nephrol. 2016; 12: 610–623. - PubMed
-
- Bansal N, Zelnick L, Bhat Z, Dobre M, He J, Lash J, Jaar B, Mehta R, Raj D, Rincon‐Choles H, Saunders M, Schrauben S, Weir M, Wright J, Go AS, CRIC Study Investigators . Burden and outcomes of heart failure hospitalizations in adults with chronic kidney disease. J Am Coll Cardiol. 2019; 73: 2691–2700. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
