

Friedreich ataxia: clinical features and new developments
- PMID: 35766110
- PMCID: PMC9517959
- DOI: 10.2217/nmt-2022-0011
Friedreich ataxia: clinical features and new developments
Abstract
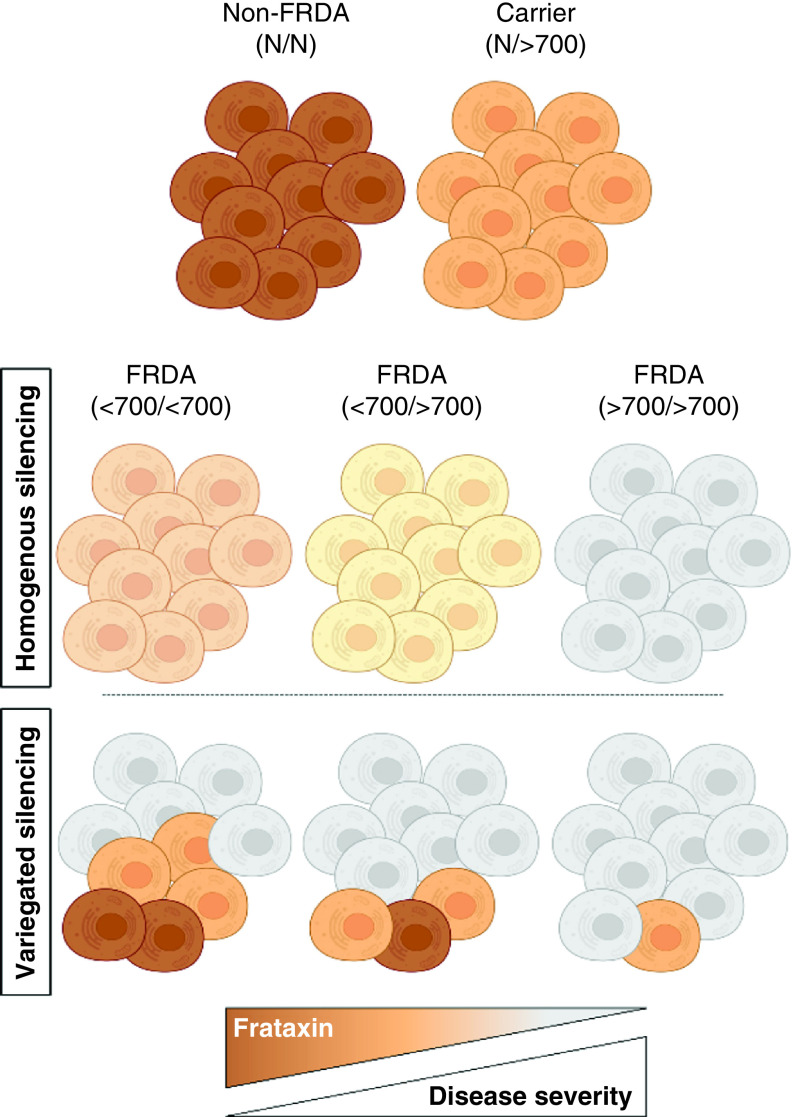
Friedreich's ataxia (FRDA), a neurodegenerative disease characterized by ataxia and other neurological features, affects 1 in 50,000-100,000 individuals in the USA. However, FRDA also includes cardiac, orthopedic and endocrine dysfunction, giving rise to many secondary disease characteristics. The multifaceted approach for clinical care has necessitated the development of disease-specific clinical care guidelines. New developments in FRDA include the advancement of clinical drug trials targeting the NRF2 pathway and frataxin restoration. Additionally, a novel understanding of gene silencing in FRDA, reflecting a variegated silencing pattern, will have applications to current and future therapeutic interventions. Finally, new perspectives on the neuroanatomy of FRDA and its developmental features will refine the time course and anatomical targeting of novel approaches.
Keywords: Frataxin; NRF2; antioxidant; clinical care guideline; clinical trial; multisystem.
Plain language summary
Friedreich's ataxia (FRDA), mainly referred to as a disorder of balance, is characterized by loss of coordination (ataxia) in the arms and legs and other neurological features, affecting about 1 in 50,000 people in the USA. FRDA also includes serious heart disease, aggressive scoliosis, diabetes and many other disease characteristics. Due to various clinical care needs, disease-specific clinical care guidelines have been created. New developments in FRDA include the advancement of clinical drug trials targeting cell signaling pathways and restoration of the deficient protein found in individuals with FRDA. Additionally, a new understanding of the role of the various genetic factors that contribute to the development of FRDA could affect current and future therapies. Finally, new perspectives on the early developmental features of FRDA will help refine the time course and accelerate new treatments.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical