

Association between hypotension during 24 h ambulatory blood pressure monitoring and reflex syncope: the SynABPM 1 study
- PMID: 35766175
- PMCID: PMC9553097
- DOI: 10.1093/eurheartj/ehac347
Association between hypotension during 24 h ambulatory blood pressure monitoring and reflex syncope: the SynABPM 1 study
Abstract
Aims: Diagnostic criteria for ambulatory blood pressure monitoring (ABPM) in patients with suspected reflex syncope are lacking. The study hypothesis was that patients with reflex syncope have a higher prevalence of systolic blood pressure (SBP) drops on ABPM.
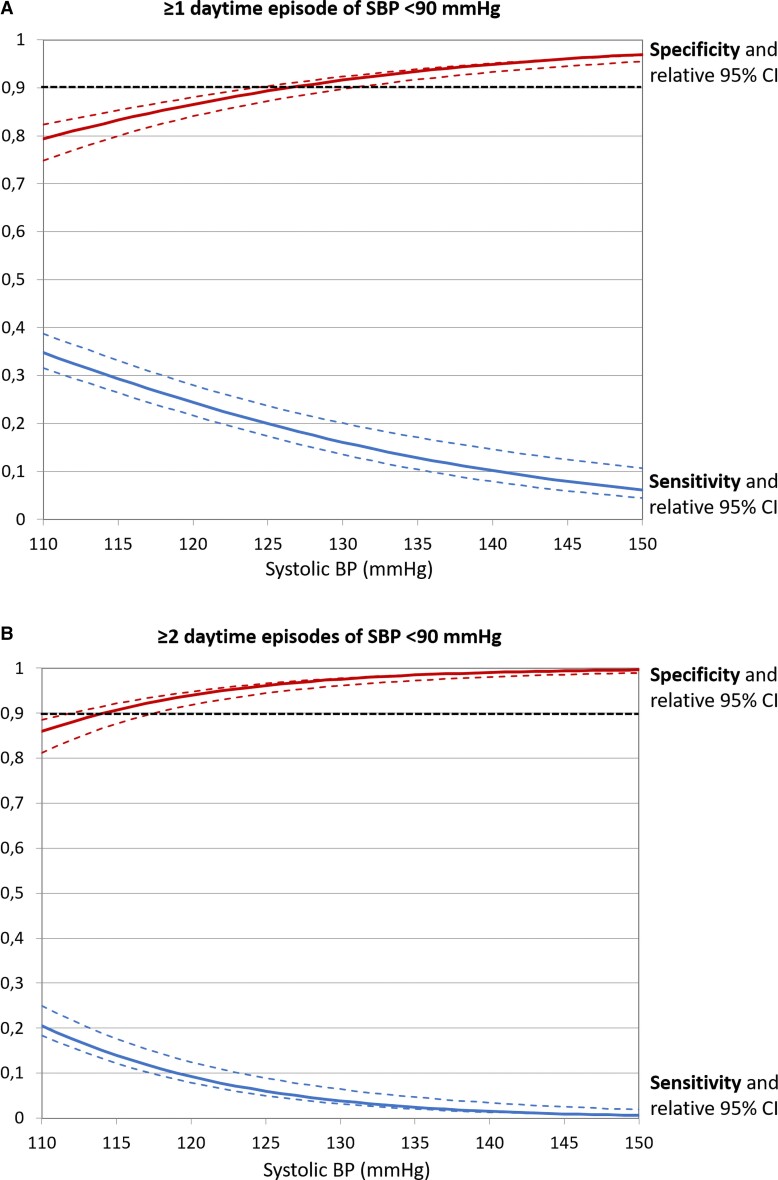
Methods and results: ABPM data from reflex syncope patients and controls, matched by average 24 h SBP, age, sex, and hypertension were compared. Patients with constitutional hypotension, orthostatic hypotension, and predominant cardioinhibition during carotid sinus massage or prolonged electrocardiogram monitoring or competing causes of syncope were excluded. Daytime and nighttime SBP drops (<110, 100, 90, 80 mmHg) were assessed. Findings were validated in an independent sample. In the derivation sample, daytime SBP drops were significantly more common in 158 syncope patients than 329 controls. One or more daytime drops <90 mmHg achieved 91% specificity and 32% sensitivity [odds ratio (OR) 4.6, P < 0.001]. Two or more daytime drops <100 mmHg achieved 84% specificity and 40% sensitivity (OR 3.5, P = 0.001). Results were confirmed in the validation sample of 164 syncope patients and 164 controls: one or more daytime SBP drops <90 mmHg achieved 94% specificity and 29% sensitivity (OR 6.2, P < 0.001), while two or more daytime SBP drops <100 mmHg achieved 83% specificity and 35% sensitivity (OR 2.6, P < 0.001).
Conclusion: SBP drops during ABPM are more common in reflex syncope patients than in controls. Cut-off values that may be applied in clinical practice are defined. This study expands the current indications for ABPM to patients with reflex syncope.
Keywords: Ambulatory blood pressure; Blood pressure cut-off values; Hypotension; Hypotensive episode; Low blood pressure.
© The Author(s) 2022. Published by Oxford University Press on behalf of European Society of Cardiology.
Conflict of interest statement
Conflicts of interests: R.S. declares the following potential conflicts of interest: consulting fees from Medtronic Inc (unrelated to present work); payment for expert testimony in medico-legal cases in UK (related to syncope but unrelated to this work); member of clinical events committee for the BioSync study (published in 2021 in European Heart Journal); Secretary to the Executive Board of World Society of Arrhythmias; private shareholder receiving only dividends from Boston Scientific Corp and Edwards Lifesciences Corp. A.F. has received speaker fees from Medtronic Inc., Biotronik, and Bristol-Myers Squibb, and is consultant to Medtronic Inc, and Argenx BV. The other authors declare no conflicts of interest.
Figures



Comment in
-
The extended role of 24 h ambulatory blood pressure monitoring for reflex syncope.Eur Heart J. 2022 Oct 11;43(38):3777-3780. doi: 10.1093/eurheartj/ehac409. Eur Heart J. 2022. PMID: 35924302 No abstract available.
References
-
- Brignole M, Moya A, De Lange FJ, Deharo JC, Elliott PM, Fanciulli Aet al. . 2018 ESC guidelines for the diagnosis and management of syncope. Eur Heart J 2018;39:1883–1948. - PubMed
-
- Wenzke KE, Walsh KE, Kalscheur M, Wasmund SL, Page RL, Brignole Met al. . Clinical characteristics and outcome of patients with situational syncope compared to patients with vasovagal syncope. Pacing Clin Electrophysiol 2017;40:591–595. - PubMed
-
- Ungar A, Mussi C, Ceccofiglio A, Bellelli G, Nicosia F, Bo M, et al. . Etiology of syncope and unexplained falls in elderly adults with dementia: syncope and dementia (SYD) study. J Am Geriatr Soc 2016;64:1567–1573. - PubMed
