

Multifaceted Intervention to Improve P2Y12 Inhibitor Adherence After Percutaneous Coronary Intervention: A Stepped Wedge Trial
- PMID: 35766258
- PMCID: PMC9333389
- DOI: 10.1161/JAHA.121.024342
Multifaceted Intervention to Improve P2Y12 Inhibitor Adherence After Percutaneous Coronary Intervention: A Stepped Wedge Trial
Abstract
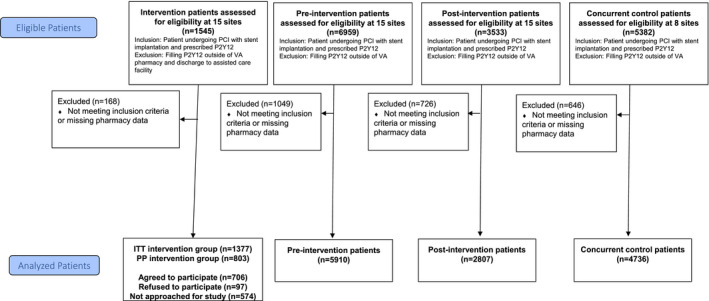
Background P2Y12 inhibitor medications are critical following percutaneous coronary intervention (PCI); however, adherence remains suboptimal. Our objective was to assess the effectiveness of a multifaceted intervention to improve P2Y12 inhibitor adherence following PCI. Methods and Results This was a modified stepped wedge trial of 52 eligible hospitals, of which 15 were randomly selected and agreed to participate (29 hospitals declined, and 8 eligible hospitals were not contacted). At each intervention hospital, patient recruitment occurred for 6 months and enrolled patients were followed up for 1 year after PCI. Three control groups were used: patients at intervention hospitals undergoing PCI (1) before the intervention period (preintervention); (2) after the intervention period (postintervention); or (3) at the 8 hospitals not contacted (concurrent controls). The intervention consisted of 4 components: (1) P2Y12 inhibitor delivered to patients' bedside after PCI; (2) education on importance of P2Y12 inhibitors; (3) automated reminder telephone calls to refill medication; and (4) outreach to patients if they delayed refilling P2Y12 inhibitor. The primary outcomes were as follows: (1) proportion of patients with delays filling P2Y12 inhibitor at hospital discharge and (2) proportion of patients who were adherent in the year after PCI using pharmacy refill data. Primary analysis compared intervention with preintervention control patients. There were 1377 (intent-to-treat) potentially eligible patients, of whom 803 (per protocol) were approached at intervention sites versus 5910 preintervention, 2807 postintervention, and 4736 concurrent control patients. In the intent-to-treat analysis, intervention patients were less likely to delay filling P2Y12 at hospital discharge (-3.4%; 98.3% CI, -1.2% to -5.6%) and more likely to be adherent to P2Y12 (4.1%; 98.3% CI, 1.0%-7.1%) at 1 year, but had more clinical events (3.2%; 98.3% CI, 2.3%-4.1%) driven by repeated PCI compared with preintervention patients. In post hoc analysis looking at myocardial infarction, stroke, and death, intervention patients had lower event rates compared with preintervention patients (-1.7%; 98.3% CI, -2.3% to -1.1%). Conclusions A 4-component intervention targeting P2Y12 inhibitor adherence was difficult to implement. The intervention produced mixed results. It improved P2Y12 adherence, but there was also an increase in repeat PCI. Registration URL: https://www.clinicaltrials.gov; Unique identifier: NCT01609842.
Keywords: P2Y12 inhibitor; clinical trial; medication adherence.
Figures
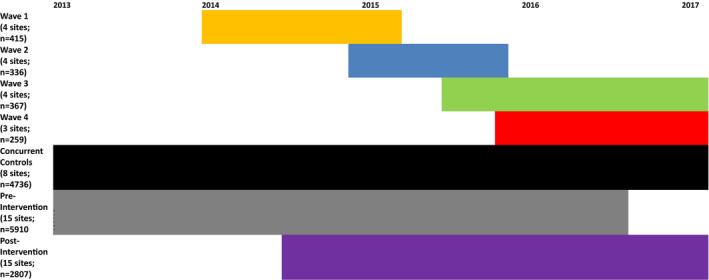
Intervention sites: hospitals performing at least 20 percutaneous coronary intervention (PCI) procedures annually between October 1, 2009, and September 30, 2012, were grouped into quintiles based on the proportion of patients who delayed P2Y12 inhibitor pick up during those years at each hospital. Hospitals in the quintile with the lowest proportion (quintile 1) of patients with P2Y12 inhibitor fill delay were excluded from randomization to the intervention because they had little room to improve. Within each of the remaining 4 strata (quintiles 2–5), 4 hospitals were randomized to each of the 4 intervention waves. Hospitals that declined participation in any wave were replaced by another randomly selected hospital from the same stratum. There were 3 waves with 4 hospitals in each wave. In the fourth wave, none of the hospitals in quintile 4 agreed to implement the intervention, so only 3 sites implemented the intervention, resulting in a total of 15 intervention sites. The 8 sites remaining in the 4 strata that were eligible but not approached to participate served as concurrent control sites.
Preintervention period: patients undergoing PCI who were treated at an intervention hospital before the 6‐month intervention period.
Postintervention period: patients undergoing PCI who were treated at an intervention hospital after the intervention period ended.
Concurrent controls: patients undergoing PCI and treated at hospitals that were eligible to participate in the intervention but were not invited to implement the intervention because enough hospitals within that stratum had already agreed to participate.
Comment in
-
Translating Clinical Guidelines Into Care Delivery Innovation: The Importance of Rigorous Methods for Generating Evidence.J Am Heart Assoc. 2022 Jul 5;11(13):e026677. doi: 10.1161/JAHA.122.026677. Epub 2022 Jun 29. J Am Heart Assoc. 2022. PMID: 35766287 Free PMC article. No abstract available.
References
-
- Benjamin EJ, Muntner P, Alonso A, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Chang AR, Cheng S, Das SR, et al. on behalf of the American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee . Heart disease and stroke statistics—2019 update: a report from the American Heart Association. Circulation. 2019;139:e56–e528. doi: 10.1161/CIR.0000000000000659 - DOI - PubMed
-
- Levine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B, Chambers CE, Ellis SG, Guyton RA, Hollenberg SM, et al. 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation. 2011;124:e574–e651. doi: 10.1161/CIR.0b013e31823ba622 - DOI - PubMed
-
- Ho PM, Tsai TT, Maddox TM, Powers JD, Carroll NM, Jackevicius C, Go AS, Margolis KL, DeFor TA, Rumsfeld JS, et al. Delays in filling clopidogrel prescription after hospital discharge and adverse outcomes after drug‐eluting stent implantation: implications for transitions of care. Circ Cardiovasc Qual Outcomes. 2010;3:261–266. doi: 10.1161/CIRCOUTCOMES.109.902031 - DOI - PubMed
-
- Tuppin P, Neumann A, Danchin N, de Peretti C, Weill A, Ricordeau P, Allemand H. Evidence‐based pharmacotherapy after myocardial infarction in France: adherence‐associated factors and relationship with 30‐month mortality and rehospitalization. Arch Cardiovasc Dis. 2010;103:363–375. doi: 10.1016/j.acvd.2010.05.003 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
