

Hemodynamic phenotype-based, capillary refill time-targeted resuscitation in early septic shock: The ANDROMEDA-SHOCK-2 Randomized Clinical Trial study protocol
- PMID: 35766659
- PMCID: PMC9345585
- DOI: 10.5935/0103-507X.20220004-pt
Hemodynamic phenotype-based, capillary refill time-targeted resuscitation in early septic shock: The ANDROMEDA-SHOCK-2 Randomized Clinical Trial study protocol
Abstract
Background: Early reversion of sepsis-induced tissue hypoperfusion is essential for survival in septic shock. However, consensus regarding the best initial resuscitation strategy is lacking given that interventions designed for the entire population with septic shock might produce unnecessary fluid administration. This article reports the rationale, study design and analysis plan of the ANDROMEDA-2 study, which aims to determine whether a peripheral perfusion-guided strategy consisting of capillary refill time-targeted resuscitation based on clinical and hemodynamic phenotypes is associated with a decrease in a composite outcome of mortality, time to organ support cessation, and hospital length of stay compared to standard care in patients with early (< 4 hours of diagnosis) septic shock.
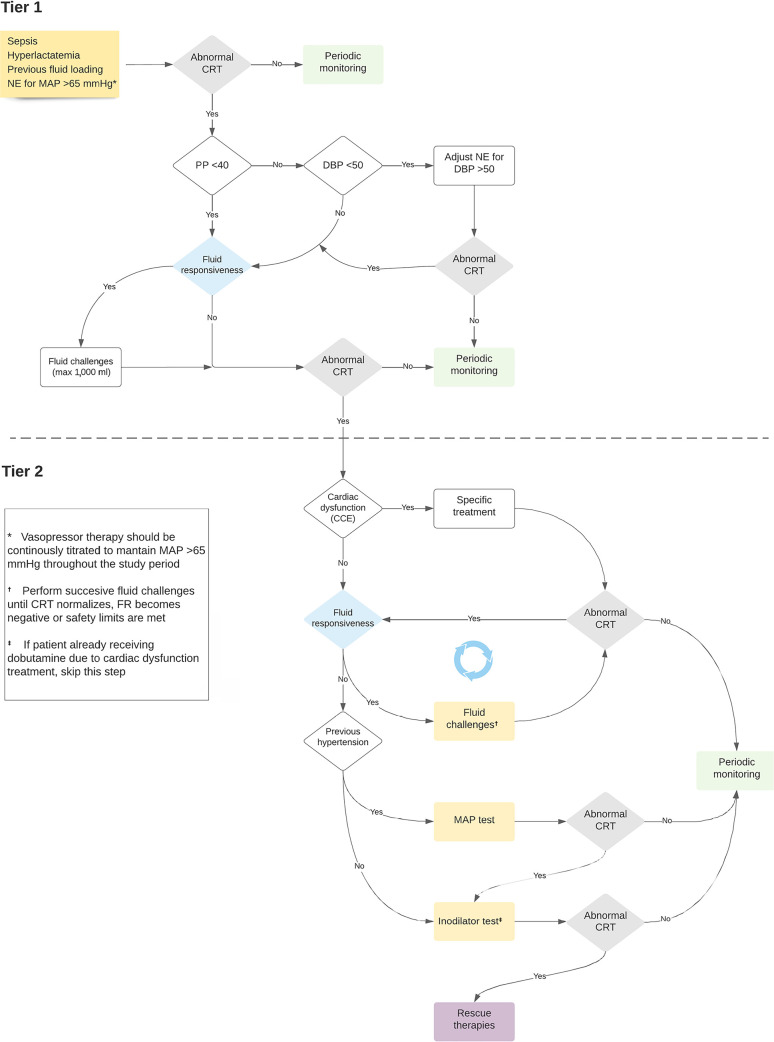
Methods: The ANDROMEDA-2 study is a multicenter, multinational randomized controlled trial. In the intervention group, capillary refill time will be measured hourly for 6 hours. If abnormal, patients will enter an algorithm starting with pulse pressure assessment. Patients with pulse pressure less than 40mmHg will be tested for fluid responsiveness and receive fluids accordingly. In patients with pulse pressure > 40mmHg, norepinephrine will be titrated to maintain diastolic arterial pressure > 50mmHg. Patients who fail to normalize capillary refill time after the previous steps will be subjected to critical care echocardiography for cardiac dysfunction evaluation and subsequent management. Finally, vasopressor and inodilator tests will be performed to further optimize perfusion. A sample size of 1,500 patients will provide 88% power to demonstrate superiority of the capillary refill time-targeted strategy.
Conclusions: If hemodynamic phenotype-based, capillary refill time-targeted resuscitation demonstrates to be a superior strategy, care processes in septic shock resuscitation can be optimized with bedside tools.
Introdução: A reversão precoce da hipoperfusão tecidual induzida é essencial para a sobrevida no choque séptico. No entanto, falta consenso sobre a melhor estratégia de ressuscitação inicial, uma vez que intervenções destinadas a toda a população com choque séptico podem produzir administração desnecessária de líquidos. Este artigo relata a justificativa, o delineamento e o plano de análise do estudo ANDROMEDA-2, que visa determinar se uma estratégia guiada por perfusão periférica, que consiste na ressuscitação guiada pelo tempo de enchimento capilar com base em fenótipos clínicos e hemodinâmicos, está associada a uma diminuição no desfecho composto de mortalidade, tempo até a interrupção ao suporte de órgãos e tempo de internação em comparação com o atendimento padrão em pacientes com choque séptico precoce (< 4 horas do diagnóstico).
Metódos: O estudo ANDROMEDA-2 é um ensaio clínico randomizado controlado multinacional e multicêntrico. No grupo de intervenção, o tempo de enchimento capilar será medido a cada hora, durante 6 horas. Se estiver anormal, os pacientes serão alocados em um algoritmo, começando com a avaliação da pressão de pulso. Pacientes com pressão de pulso inferior a 40mmHg serão testados quanto à capacidade de resposta a líquidos e receberão líquidos de acordo. Em pacientes com pressão de pulso > 40mmHg, norepinefrina será titulada para manter a pressão arterial diastólica > 50mmHg. Os pacientes que não normalizarem o tempo de enchimento capilar após as etapas anteriores serão submetidos à ecocardiografia de cuidados intensivos para avaliação da disfunção cardíaca e posterior manejo. Por fim, serão realizados testes com vasopressores e inodilatadores para otimizar ainda mais a perfusão. Um tamanho de amostra de 1.500 pacientes fornecerá 88% de poder para demonstrar a superioridade da estratégia direcionada ao tempo de enchimento capilar.
Conclusão: Se for demonstrado que o direcionamento ao tempo de enchimento capilar é uma estratégia melhor, os processos de atendimento na ressuscitação do choque séptico podem ser otimizados com ferramentas usadas à beira do leito.
Trial registration: ClinicalTrials.gov NCT05057611.
Conflict of interest statement
Figures
References
-
- Cecconi M, Evans L, Levy M, Rhodes A. Sepsis and septic shock. Lancet. 2018;392(10141):75–87. - PubMed
-
- Sakr Y, Rubatto Birri PN, Kotfis K, Nanchal R, Shah B, Kluge S, Schroeder ME, Marshall JC, Vincent JL, Intensive Care Over Nations Investigators Higher fluid balance increases the risk of death from sepsis: results from a large international audit. Crit Care Med. 2017;45(3):386–394. - PubMed
-
- Hernández G, Ospina-Tascón GA, Damiani LP, Estenssoro E, Dubin A, Hurtado J, et al. Effect of a Resuscitation Strategy Targeting Peripheral Perfusion Status vs Serum Lactate Levels on 28-Day Mortality Among Patients With Septic Shock: The ANDROMEDA-SHOCK Randomized Clinical Trial. JAMA. 2019;321(7):654–664. - PMC - PubMed
-
- Zampieri FG, Damiani LP, Bakker J, Ospina-Tascón GA, Castro R, Cavalcanti AB, et al. Effects of a Resuscitation Strategy Targeting Peripheral Perfusion Status versus Serum Lactate Levels among Patients with Septic Shock. A Bayesian Reanalysis of the ANDROMEDA-SHOCK Trial. Am J Respir Crit Care Med. 2020;201(4):423–429. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
