

Effect of electrophysical resources on healing of neurotendinous injury in an experimental model of type I diabetes and kidney disease
- PMID: 35766669
- PMCID: PMC9239559
- DOI: 10.1590/acb370402
Effect of electrophysical resources on healing of neurotendinous injury in an experimental model of type I diabetes and kidney disease
Abstract
Purpose: To evaluate and describe the effect of electrophysical resources laser therapy (LLLT), intravascular laser blood irradiation (ILIB), and cryotherapy on the healing process of neurotendinous injury, as well as possible systemic changes, in the experimental model of type 1 diabetes associated with kidney injury.
Methods: The animals were randomized into four groups: G1) healthy control with untreated injury; G2) healthy control with injury and treatment; G3) disease control with untreated lesion; G4) disease with injury and treatment. Furthermore, the treated groups were divided into three, according to the type of treatment. All animals were induced to neurotendinous injury and treated according to the therapeutic protocols. Healing and inflammation were analyzed by semiquantitative histopathological study.
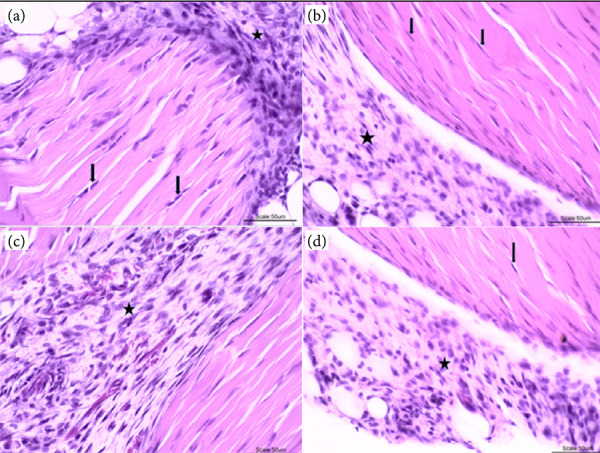
Results: It was observed in sick animals treated with cryotherapy and ILIB reduction of inflammatory exudate, presence of fibroblasts and organization of collagen, when compared to the effects of LLLT. Moreover, there was reduction in glycemic levels in the group treated with ILIB.
Conclusions: Cryotherapy promoted reduction in inflammatory exudate and organization of collagen fibers, in addition to the absence of signs of tissue necrosis, in the groups treated with and without the disease. ILIB therapy showed the same findings associated with significant reduction in glycemic levels in the group of diseased animals. The application of LLLT showed increased inflammatory exudate, low organization of collagen fibers and low sign of tissue degeneration and necrosis. This study in a model of associated diseases (diabetes and kidney disease) whose effects of electrophysical resources studied after neurotendinous injury allows us to verify histopathological variables suggestive of patients with the same comorbidities.
Conflict of interest statement
Conflict of interest: Nothing to declare.
Figures








Similar articles
-
The effects of transcutaneous low-level laser therapy on the skin healing process: an experimental model.Lasers Med Sci. 2018 Jul;33(5):967-976. doi: 10.1007/s10103-017-2429-x. Epub 2018 Jan 6. Lasers Med Sci. 2018. PMID: 29306974
-
Quercetin and low level laser therapy promote wound healing process in diabetic rats via structural reorganization and modulatory effects on inflammation and oxidative stress.Biomed Pharmacother. 2018 May;101:58-73. doi: 10.1016/j.biopha.2018.02.040. Epub 2018 Feb 22. Biomed Pharmacother. 2018. PMID: 29477473
-
LLLT improves tendon healing through increase of MMP activity and collagen synthesis.Lasers Med Sci. 2013 Sep;28(5):1281-8. doi: 10.1007/s10103-012-1236-7. Epub 2012 Nov 21. Lasers Med Sci. 2013. PMID: 23179310
-
ILIB (intravascular laser irradiation of blood) as an adjuvant therapy in the treatment of patients with chronic systemic diseases-an integrative literature review.Lasers Med Sci. 2020 Dec;35(9):1899-1907. doi: 10.1007/s10103-020-03100-4. Epub 2020 Jul 12. Lasers Med Sci. 2020. PMID: 32656732 Review.
-
Intravascular laser irradiation of blood (ILIB) used to treat lung diseases: a short critical review.Lasers Med Sci. 2023 Mar 25;38(1):93. doi: 10.1007/s10103-023-03750-0. Lasers Med Sci. 2023. PMID: 36964849 Free PMC article. Review.
References
-
- Denadai AS, Aydos RD, Silva IS, Olmedo L, Cardoso BM, Silva BA, et al. Acute effects of low-level laser therapy (660 nm) on oxidative stress levels in diabetic rats with skin wounds. J Exp Ther Oncol. 2017;11(2):85–89. - PubMed
-
- Nascimento OJ, Pupe CC, Cavalcanti EB. Neuropatia diabética. Rev Dor. 2016;17(Supl. 1):46–51. doi: 10.5935/1806-0013.20160047. - DOI
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
