

Challenges of variant reinterpretation: Opinions of stakeholders and need for guidelines
- PMID: 35767006
- PMCID: PMC10407574
- DOI: 10.1016/j.gim.2022.06.002
Challenges of variant reinterpretation: Opinions of stakeholders and need for guidelines
Abstract
Purpose: The knowledge used to classify genetic variants is continually evolving, and the classification can change on the basis of newly available data. Although up-to-date variant classification is essential for clinical management, reproductive planning, and identifying at-risk family members, there is no consistent practice across laboratories or clinicians on how or under what circumstances to perform variant reinterpretation.
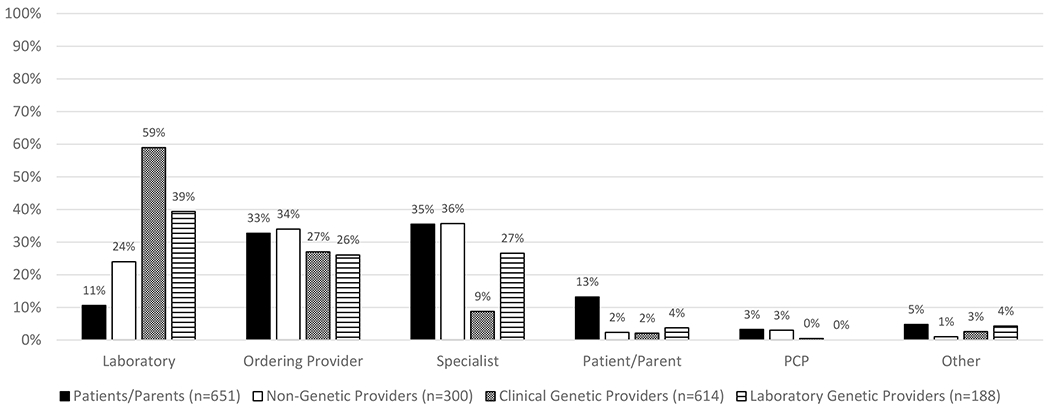
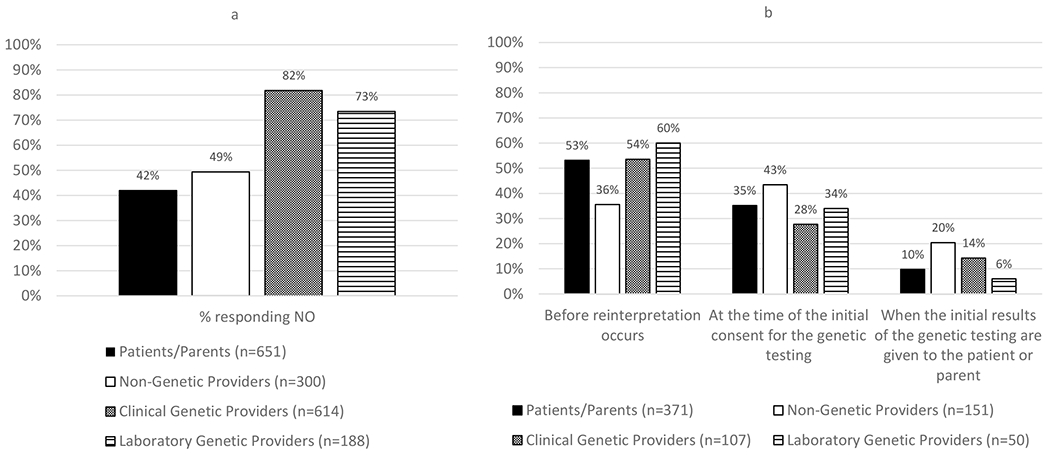
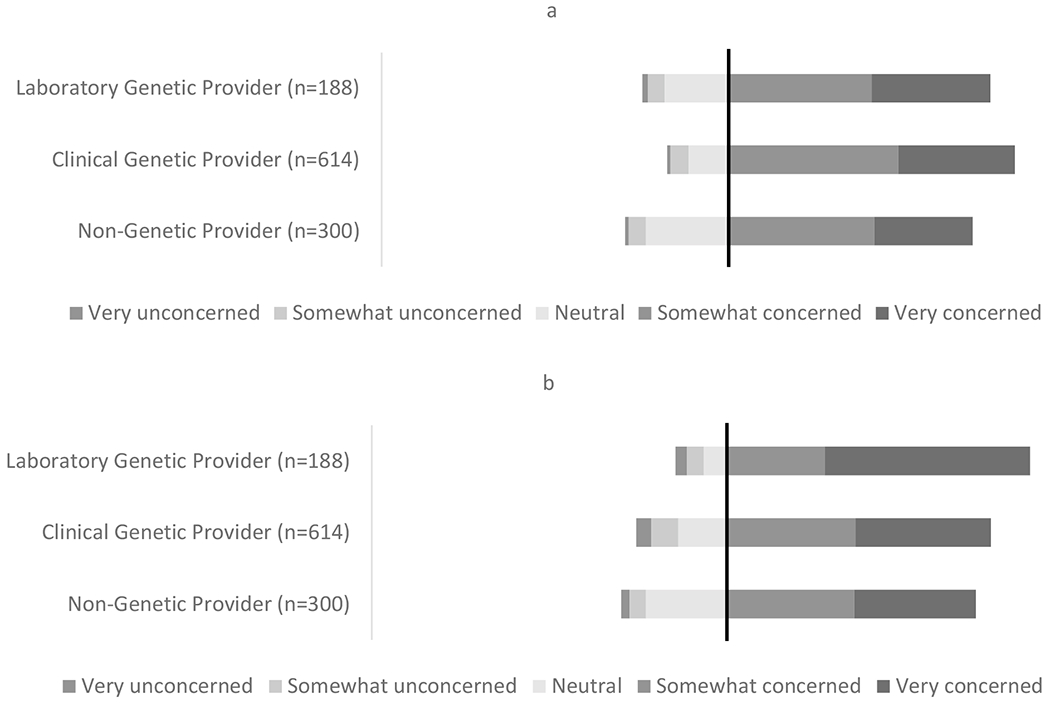
Methods: We conducted exploratory focus groups (N = 142) and surveys (N = 1753) with stakeholders involved in the process of variant reinterpretation (laboratory directors, clinical geneticists, genetic counselors, nongenetic providers, and patients/parents) to assess opinions on key issues, including initiation of reinterpretation, variants to report, termination of the responsibility to reinterpret, and concerns about consent, cost, and liability.
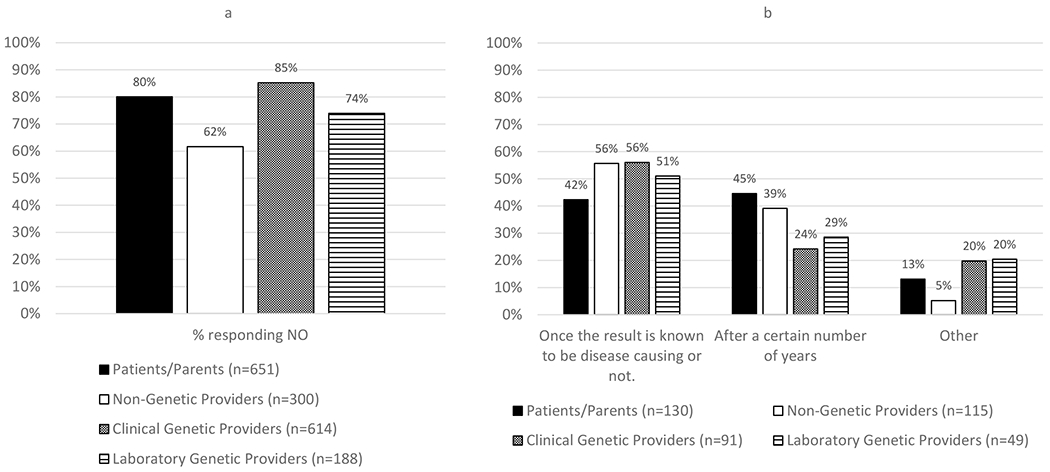
Results: Stakeholders widely agreed that there should be no fixed termination point to the responsibility to reinterpret a previously reported genetic variant. There were significant concerns about liability and lack of agreement about many logistical aspects of variant reinterpretation.
Conclusion: Our findings suggest a need to (1) develop consensus and (2) create transparency and awareness about the roles and responsibilities of parties involved in variant reinterpretation. These data provide a foundation for developing guidelines on variant reinterpretation that can aid in the development of a low-cost, scalable, and accessible approach.
Keywords: Genetic testing; Liability; Variant of uncertain significance; Variant reclassification; Variant reinterpretation.
Copyright © 2022 American College of Medical Genetics and Genomics. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest W.K.C. is on the Regeneron Genetics Center Scientific Advisory Board and the Board of Directors of Prime Medicine. The other authors declare no conflicts of interest.
Figures
References
-
- Richards S, Aziz N, Bale S, Bick D, Das S, Gastier-Foster J, et al. Standards and guidelines for the interpretation of sequence variants: A joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med. 2015;17(5):405–24. - PMC - PubMed
-
- Caswell-Jin JL, Gupta T, Hall E, Petrovchich IM, Mills MA, Kingham KE, et al. Racial/ethnic differences in multiple-gene sequencing results for hereditary cancer risk. Genet Med. 2018;20(2):234–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
