

Malaria Transmission Dynamics in a High-Transmission Setting of Western Kenya and the Inadequate Treatment Response to Artemether-Lumefantrine in an Asymptomatic Population
- PMID: 35767269
- PMCID: PMC9938745
- DOI: 10.1093/cid/ciac527
Malaria Transmission Dynamics in a High-Transmission Setting of Western Kenya and the Inadequate Treatment Response to Artemether-Lumefantrine in an Asymptomatic Population
Abstract
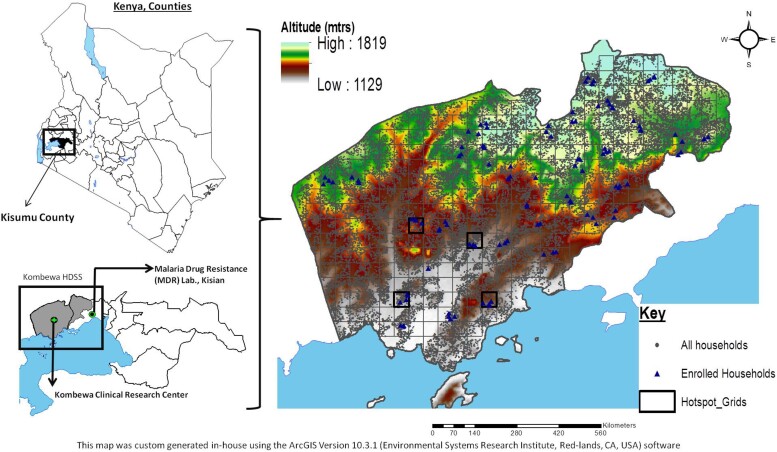
Background: Assessing the infectious reservoir is critical in malaria control and elimination strategies. We conducted a longitudinal epidemiological study in a high-malaria-burden region in Kenya to characterize transmission in an asymptomatic population.
Methods: 488 study participants encompassing all ages in 120 households within 30 clusters were followed for 1 year with monthly sampling. Malaria was diagnosed by microscopy and molecular methods. Transmission potential in gametocytemic participants was assessed using direct skin and/or membrane mosquito feeding assays, then treated with artemether-lumefantrine. Study variables were assessed using mixed-effects generalized linear models.
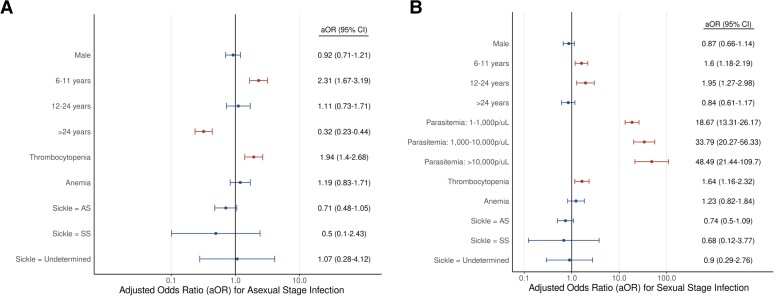
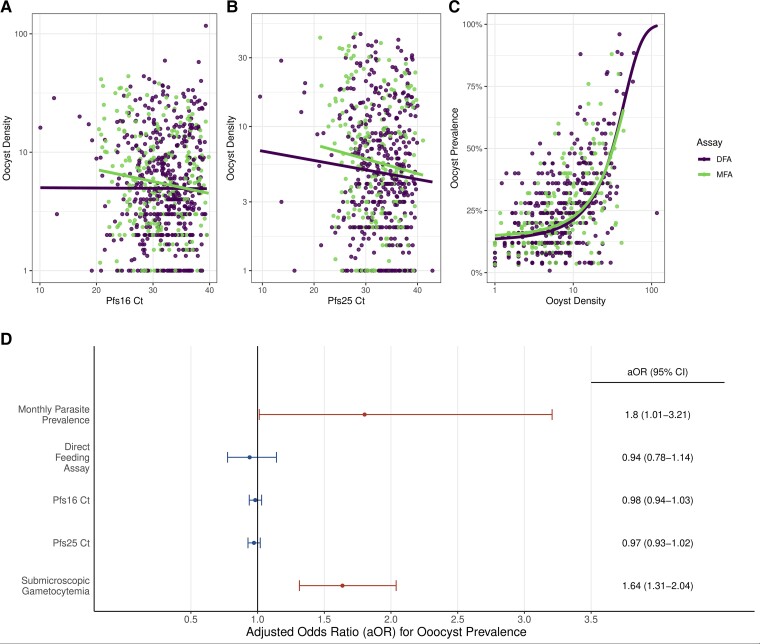
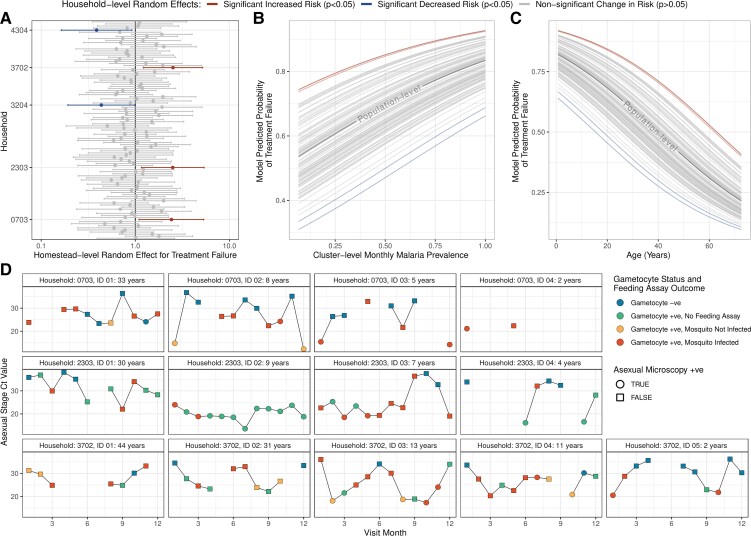
Results: Asexual and sexual parasite data were collected from 3792 participant visits, with 903 linked with feeding assays. Univariate analysis revealed that the 6-11-year-old age group was at higher risk of harboring asexual and sexual infections than those <6 years old (odds ratio [OR] 1.68, P < .001; and OR 1.81, P < .001), respectively. Participants with submicroscopic parasitemia were at a lower risk of gametocytemia compared with microscopic parasitemia (OR 0.04, P < .001), but they transmitted at a significantly higher rate (OR 2.00, P = .002). A large proportion of the study population who were infected at least once remained infected (despite treatment) with asexual (71.7%, 291/406) or sexual (37.4%, 152/406) parasites. 88.6% (365/412) of feeding assays conducted in individuals who failed treatment the previous month resulted in transmissions.
Conclusions: Individuals with asymptomatic infection sustain the transmission cycle, with the 6-11-year age group serving as an important reservoir. The high rates of artemether-lumefantrine treatment failures suggest surveillance programs using molecular methods need to be expanded for accurate monitoring and evaluation of treatment outcomes.
Keywords: Plasmodium falciparum; artemether/lumefantrine; drug resistance; malaria control and elimination; malaria surveillance and transmission dynnamics.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. The authors: No reported conflicts of interest. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
Comment in
-
How to Interpret Parasite Persistence and Transmission to Mosquitoes After Antimalarial Treatment in Kenya?Clin Infect Dis. 2023 Feb 8;76(3):555-557. doi: 10.1093/cid/ciac740. Clin Infect Dis. 2023. PMID: 36069392 No abstract available.
References
-
- Nahlen BL, Low-Beer D. Building to collective impact: the global fund support for measuring reduction in the burden of malaria. Am J Trop Med Hyg 2007; 77:321–7. - PubMed
-
- Stone W, Goncalves BP, Bousema T, Drakeley C. Assessing the infectious reservoir of falciparum malaria: past and future. Trends Parasitol 2015; 31:287–96. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
