

Systemic and Oligo-Acquired Resistance to PD-(L)1 Blockade in Lung Cancer
- PMID: 35767426
- PMCID: PMC10448606
- DOI: 10.1158/1078-0432.CCR-22-0657
Systemic and Oligo-Acquired Resistance to PD-(L)1 Blockade in Lung Cancer
Abstract
Purpose: Clinical patterns and the associated optimal management of acquired resistance to PD-(L)1 blockade are poorly understood.
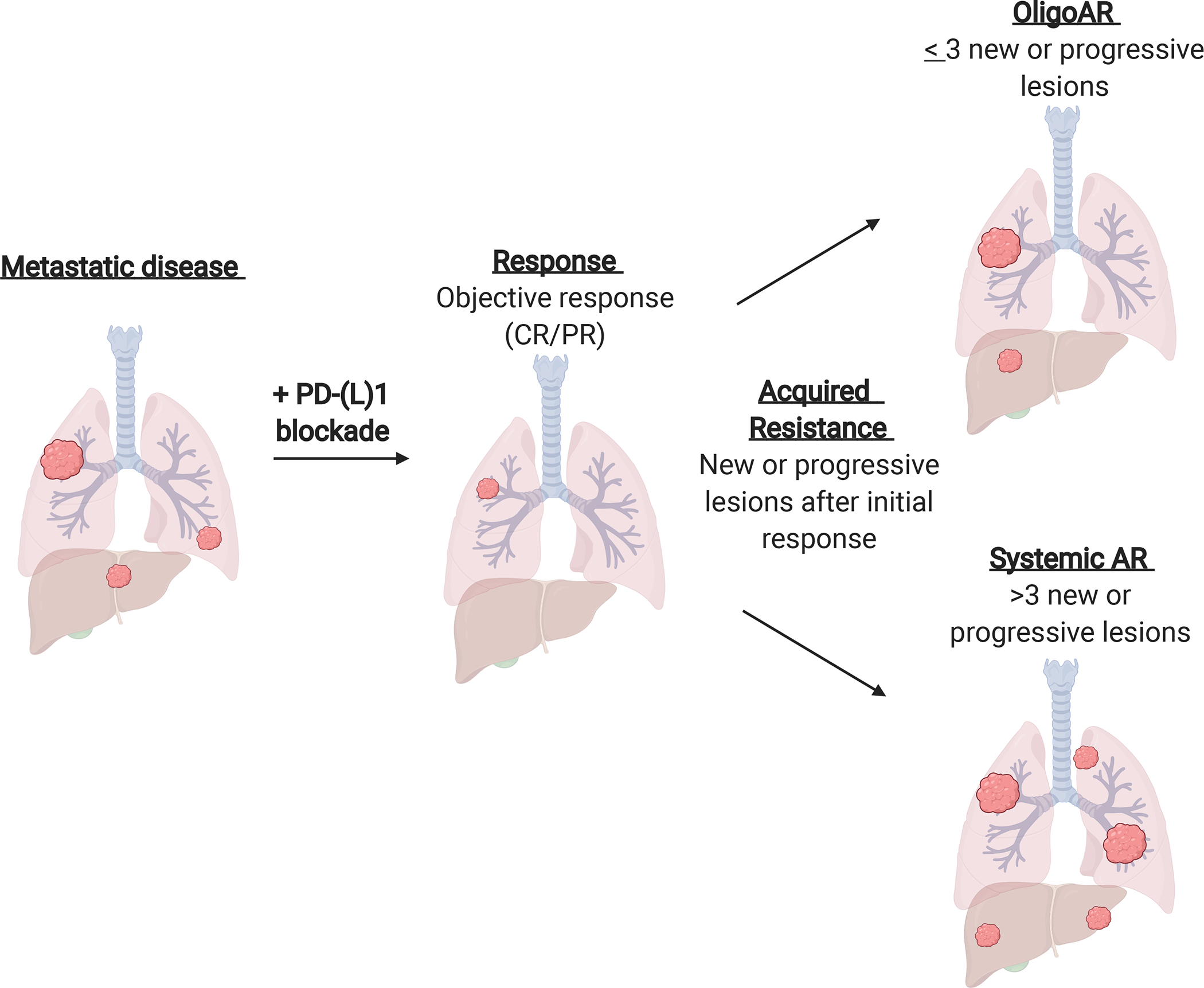
Experimental design: All cases of metastatic lung cancer treated with PD-(L)1 blockade at Memorial Sloan Kettering were reviewed. In acquired resistance (complete/partial response per RECIST, followed by progression), clinical patterns were distinguished as oligo (OligoAR ≤ 3 lesions of disease progression) or systemic (sAR). We analyzed the relationships between patient characteristics, burden/location of disease, outcomes, and efficacy of therapeutic interventions.
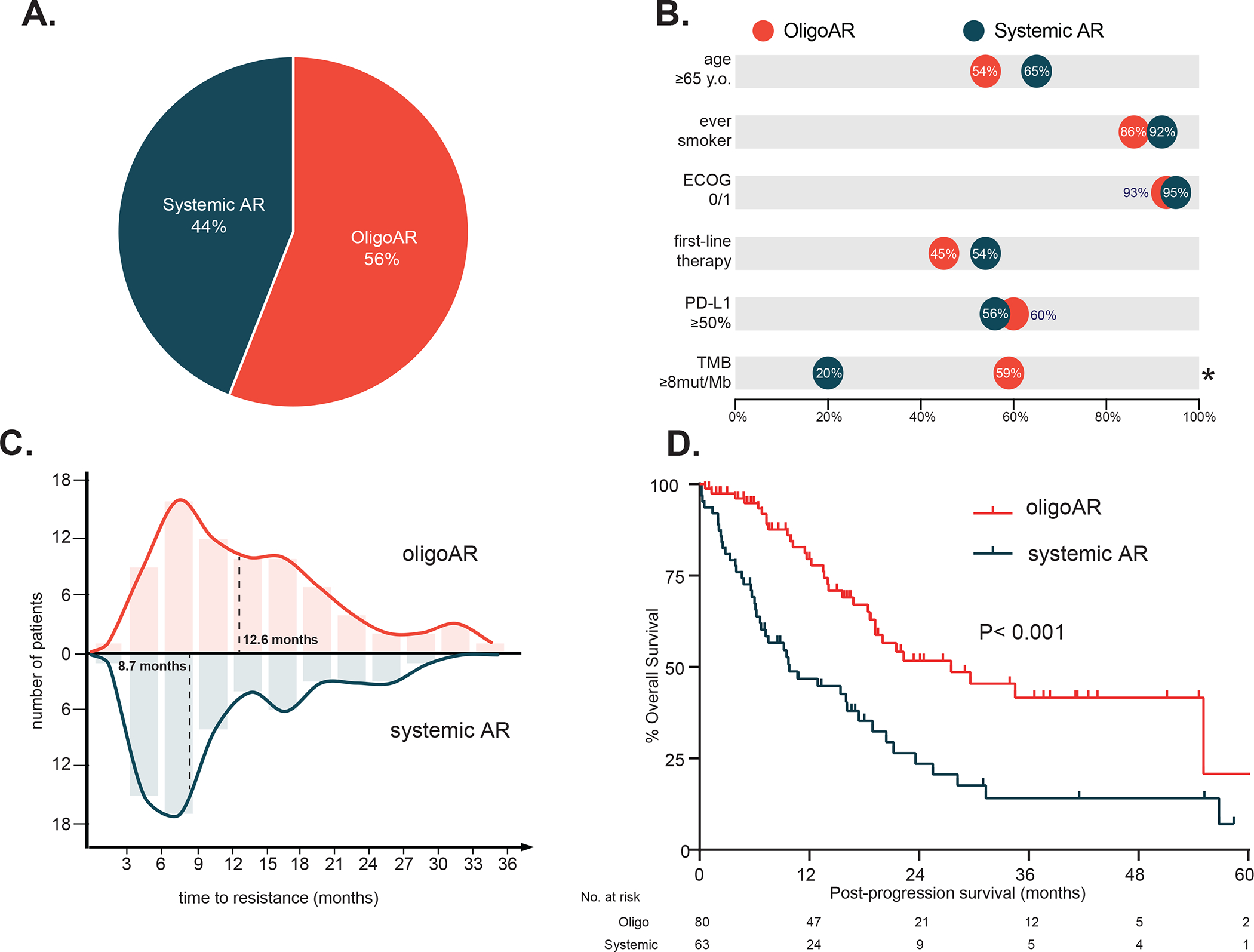
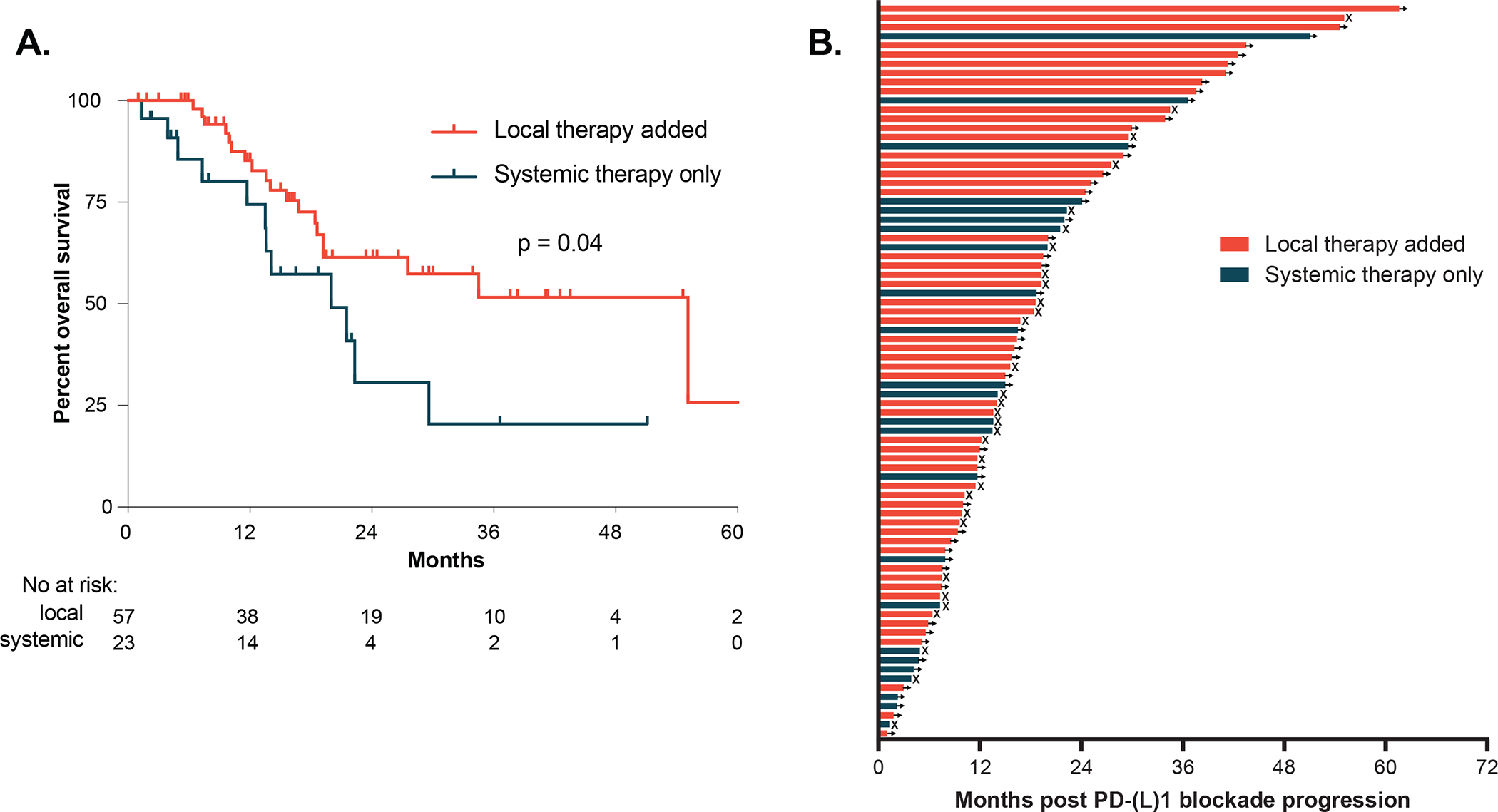
Results: Of 1,536 patients, 312 (20%) had an initial response and 143 developed AR (9% overall, 46% of responders). OligoAR was the most common pattern (80/143, 56%). Baseline tumor mutational burden, depth of response, and duration of response were significantly increased in oligoAR compared with sAR (P < 0.001, P = 0.03, P = 0.04, respectively), whereas baseline PD-L1 and tumor burden were similar. Post-progression, oligoAR was associated with improved overall survival (median 28 months vs. 10 months, P < 0.001) compared with sAR. Within oligoAR, post-progression survival was greater among patients treated with locally-directed therapy (e.g., radiation, surgery; HR, 0.41; P = 0.039). Fifty-eight percent of patients with oligoAR treated with locally-directed therapy alone are progression-free at last follow-up (median 16 months), including 13 patients who are progression-free more than 2 years after local therapy.
Conclusions: OligoAR is a common and distinct pattern of acquired resistance to PD-(L)1 blockade compared with sAR. OligoAR is associated with improved post-progression survival and some cases can be effectively managed with local therapies with durable benefit.
©2022 American Association for Cancer Research.
Conflict of interest statement
Figures
Comment in
-
Prolonged disease control with local treatments in oligo-acquired resistance to immune-checkpoint inhibitors.Transl Lung Cancer Res. 2023 Jun 30;12(6):1332-1334. doi: 10.21037/tlcr-23-50. Epub 2023 May 15. Transl Lung Cancer Res. 2023. PMID: 37425415 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
