

Open Reimplementation of the BIS Algorithms for Depth of Anesthesia
- PMID: 35767469
- PMCID: PMC9481655
- DOI: 10.1213/ANE.0000000000006119
Open Reimplementation of the BIS Algorithms for Depth of Anesthesia
Abstract
Background: BIS (a brand of processed electroencephalogram [EEG] depth-of-anesthesia monitor) scores have become interwoven into clinical anesthesia care and research. Yet, the algorithms used by such monitors remain proprietary. We do not actually know what we are measuring. If we knew, we could better understand the clinical prognostic significance of deviations in the score and make greater research advances in closed-loop control or avoiding postoperative cognitive dysfunction or juvenile neurological injury. In previous work, an A-2000 BIS monitor was forensically disassembled and its algorithms (the BIS Engine) retrieved as machine code. Development of an emulator allowed BIS scores to be calculated from arbitrary EEG data for the first time. We now address the fundamental questions of how these algorithms function and what they represent physiologically.
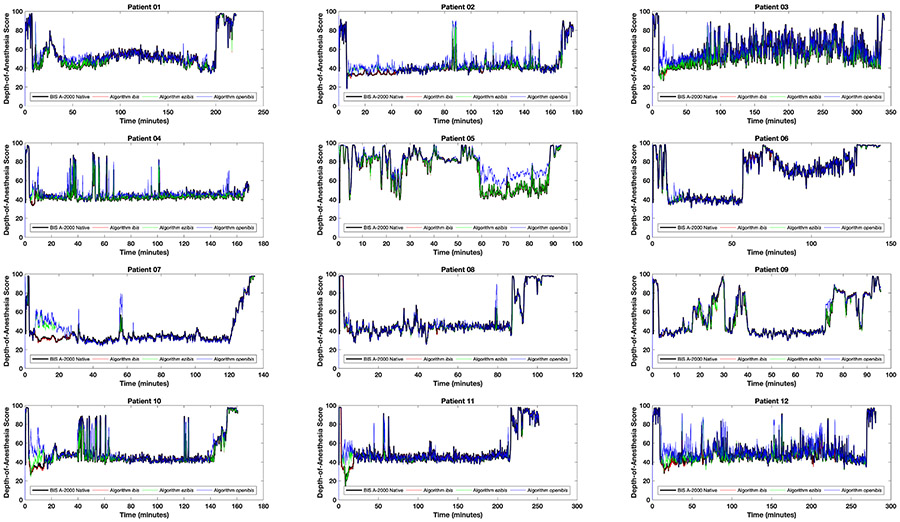
Methods: EEG data were obtained during induction, maintenance, and emergence from 12 patients receiving customary anesthetic management for orthopedic, general, vascular, and neurosurgical procedures. These data were used to trigger the closely monitored execution of the various parts of the BIS Engine, allowing it to be reimplemented in a high-level language as an algorithm entitled ibis. Ibis was then rewritten for concision and physiological clarity to produce a novel completely clear-box depth-of-anesthesia algorithm titled openibis .
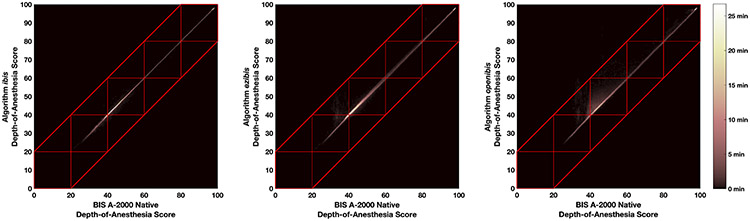
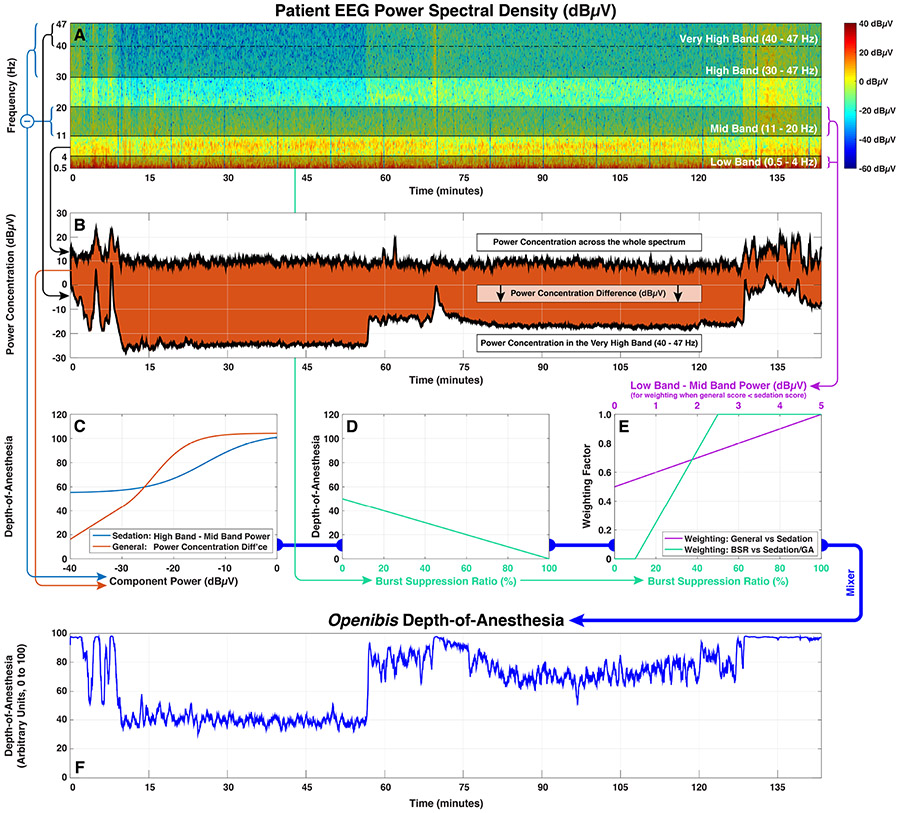
Results: The output of the ibis algorithm is functionally indistinguishable from the native BIS A-2000, with r = 0.9970 (0.9970-0.9971) and Bland-Altman mean difference between methods of -0.25 ± 2.6 on a unitless 0 to 100 depth-of-anesthesia scale. This precision exceeds the performance of any earlier attempt to reimplement the function of the BIS algorithms. The openibis algorithm also matches the output of the native algorithm very closely ( r = 0.9395 [0.9390-0.9400], Bland-Altman 2.62 ± 12.0) in only 64 lines of readable code whose function can be unambiguously related to observable features in the EEG signal. The operation of the openibis algorithm is described in an intuitive, graphical form.
Conclusions: The openibis algorithm finally provides definitive answers about the BIS: the reliance of the most important signal components on the low-gamma waveband and how these components are weighted against each other. Reverse engineering allows these conclusions to be reached with a clarity and precision that cannot be obtained by other means. These results contradict previous review articles that were believed to be authoritative: the BIS score does not appear to depend on a bispectral index at all. These results put clinical anesthesia research using depth-of-anesthesia scores on a firm footing by elucidating their physiological basis and enabling comparison to other animal models for mechanistic research.
Copyright © 2022 International Anesthesia Research Society.
Conflict of interest statement
Conflicts of Interest: See Disclosures at the end of the article.
Figures
Comment in
-
To the Editor.Anesth Analg. 2023 May 1;136(5):e21-e22. doi: 10.1213/ANE.0000000000006430. Epub 2023 Apr 14. Anesth Analg. 2023. PMID: 37058738 No abstract available.
-
On the Importance of Transparency About the Internal Operation of Medical Devices.Anesth Analg. 2023 Jun 1;136(6):e35. doi: 10.1213/ANE.0000000000006433. Epub 2023 May 19. Anesth Analg. 2023. PMID: 37205818 No abstract available.
References
-
- Brown CH, Edwards C, Lin C, Jones EL, Yanek LR, Esmaili M, Gorashi Y, Skelton R, Kaganov D, Curto R, Lessing NL, Cha S, Colantuoni E, Neufeld K, Sieber F, Dean CL, Hogue CW: Spinal Anesthesia with Targeted Sedation based on Bispectral Index Values Compared with General Anesthesia with Masked Bispectral Index Values to Reduce Delirium: The SHARP Randomized Controlled Trial. Anesthesiology 2021; 135: 992–1003 - PMC - PubMed
-
- Le Guen M, Liu N, Bourgeois E, Chazot T, Sessler DI, Rouby JJ, Fischler M: Automated sedation outperforms manual administration of propofol and remifentanil in critically ill patients with deep sedation: a randomized phase II trial. Intensive Care Med 2013; 39: 454–62 - PubMed
-
- Maheshwari A, McCormick PJ, Sessler DI, Reich DL, You J, Mascha EJ, Castillo JG, Levin MA, Duncan AE: Prolonged concurrent hypotension and low bispectral index ('double low') are associated with mortality, serious complications, and prolonged hospitalization after cardiac surgery. Br J Anaesth 2017; 119: 40–49 - PMC - PubMed
-
- Nagata O, Matsuki Y, Ogino Y, Shigemi K: Safety and efficacy of an automated anesthesia delivery system for total intravenous anesthesia with propofol, remifentanil, and rocuronium: a non-inferiority randomized controlled trial versus manually controlled anesthesia. J Anesth 2021 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
