

What will the cardiovascular disease slowdown cost? Modelling the impact of CVD trends on dementia, disability, and economic costs in England and Wales from 2020-2029
- PMID: 35767575
- PMCID: PMC9242440
- DOI: 10.1371/journal.pone.0268766
What will the cardiovascular disease slowdown cost? Modelling the impact of CVD trends on dementia, disability, and economic costs in England and Wales from 2020-2029
Abstract
Background: There is uncertainty around the health impact and economic costs of the recent slowing of the historical decline in cardiovascular disease (CVD) incidence and the future impact on dementia and disability.
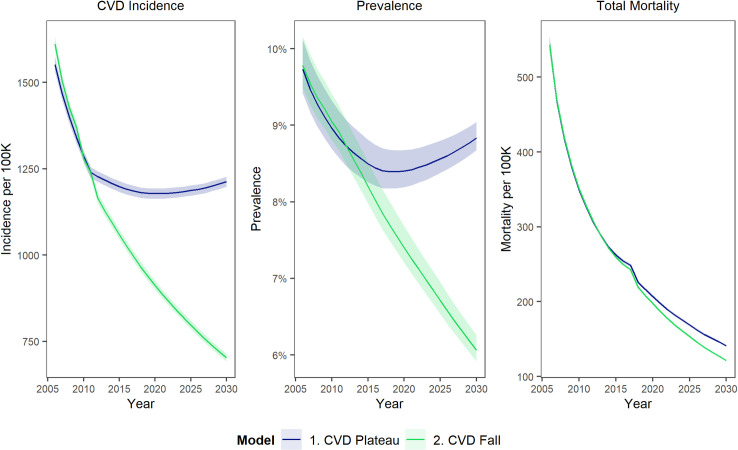
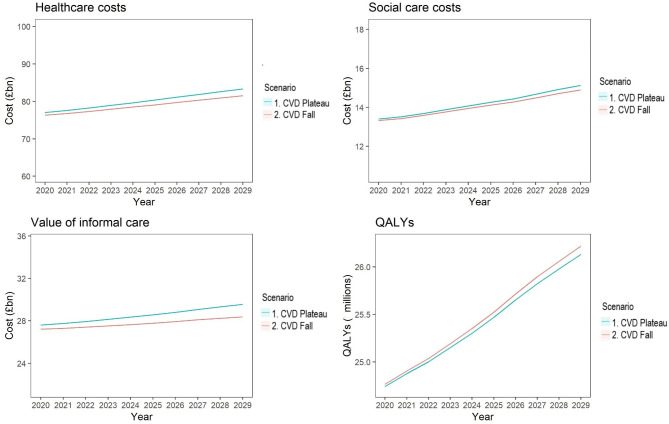
Methods: Previously validated IMPACT Better Ageing Markov model for England and Wales, integrating English Longitudinal Study of Ageing (ELSA) data for 17,906 ELSA participants followed from 1998 to 2012, linked to NHS Hospital Episode Statistics. Counterfactual design comparing two scenarios: Scenario 1. CVD Plateau-age-specific CVD incidence remains at 2011 levels, thus continuing recent trends. Scenario 2. CVD Fall-age-specific CVD incidence goes on declining, following longer-term trends. The main outcome measures were age-related healthcare costs, social care costs, opportunity costs of informal care, and quality adjusted life years (valued at £60,000 per QALY).
Findings: The total 10 year cumulative incremental net monetary cost associated with a persistent plateauing of CVD would be approximately £54 billion (95% uncertainty interval £14.3-£96.2 billion), made up of some £13 billion (£8.8-£16.7 billion) healthcare costs, £1.5 billion (-£0.9-£4.0 billion) social care costs, £8 billion (£3.4-£12.8 billion) informal care and £32 billion (£0.3-£67.6 billion) value of lost QALYs.
Interpretation: After previous, dramatic falls, CVD incidence has recently plateaued. That slowdown could substantially increase health and social care costs over the next ten years. Healthcare costs are likely to increase more than social care costs in absolute terms, but social care costs will increase more in relative terms. Given the links between COVID-19 and cardiovascular health, effective cardiovascular prevention policies need to be revitalised urgently.
Conflict of interest statement
All authors have completed the Unified Competing Interest form (available on request from the corresponding author) and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years. Dr Collins is currently on secondment as Head of Health Economics in Welsh Government; this paper does not represent any views of Welsh Government. Dr Pearson-Stuttard is also Head of Health Analytics at a commercial company, Lane Clark & Peacock LLP, vice-chair of the Royal Society for Public Health and reports personal fees from Novo Nordisk A/S, all outside of the submitted work. This work was completed as part of Dr Pearson-Stuttard’s academic appointment at Imperial College London.
Figures
References
-
- Raleigh VS. Trends in life expectancy in EU and other OECD countries: Why are improvements slowing? 2019. [cited 31 Oct 2019]. 10.1787/223159ab-en - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
