

Detection of atrial fibrillation in primary care with radial pulse palpation, electronic blood pressure measurement and handheld single-lead electrocardiography: a diagnostic accuracy study
- PMID: 35768092
- PMCID: PMC9244719
- DOI: 10.1136/bmjopen-2021-059172
Detection of atrial fibrillation in primary care with radial pulse palpation, electronic blood pressure measurement and handheld single-lead electrocardiography: a diagnostic accuracy study
Abstract
Objective: To determine the diagnostic accuracy of three tests-radial pulse palpation, an electronic blood pressure monitor and a handheld single-lead ECG device-for opportunistic screening for unknown atrial fibrillation (AF).
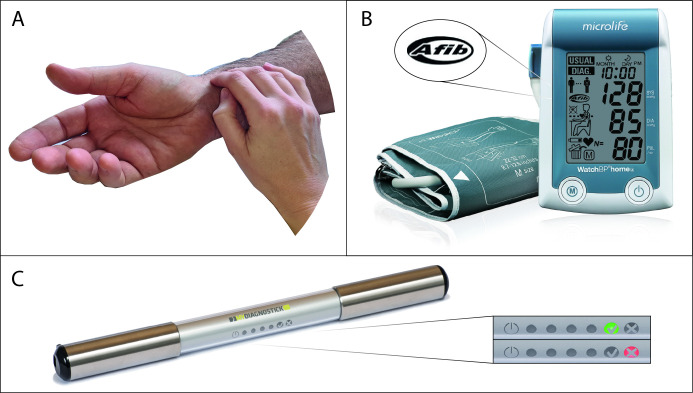
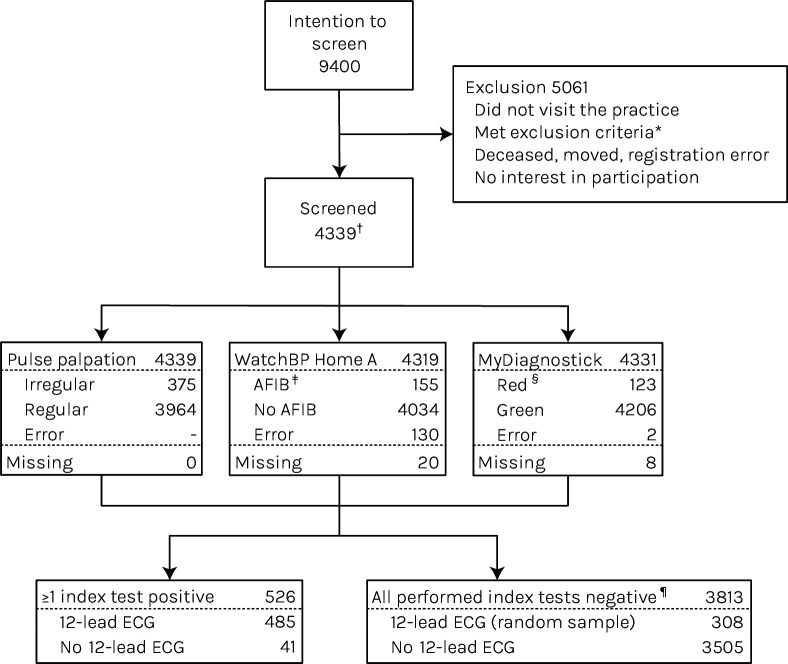
Design: We performed a diagnostic accuracy study in the intention-to-screen arm of a cluster randomised controlled trial aimed at opportunistic screening for AF in general practice. We performed radial pulse palpation, followed by electronic blood pressure measurement (WatchBP Home A) and handheld ECG (MyDiagnostick) in random order. If one or more index tests were positive, we performed a 12-lead ECG at shortest notice. Similarly, to limit verification bias, a random sample of patients with three negative index tests received this reference test. Additionally, we analysed the dataset using multiple imputation. We present pooled diagnostic parameters.
Setting: 47 general practices participated between September 2015 and August 2018.
Participants: In the electronic medical record system of the participating general practices (n=47), we randomly marked 200 patients of ≥65 years without AF. When they visited the practice for any reason, we invited them to participate. Exclusion criteria were terminal illness, inability to give informed consent or visit the practice or having a pacemaker or an implantable cardioverter-defibrillator.
Outcomes: Diagnostic accuracy of individual tests and test combinations to detect unknown AF.
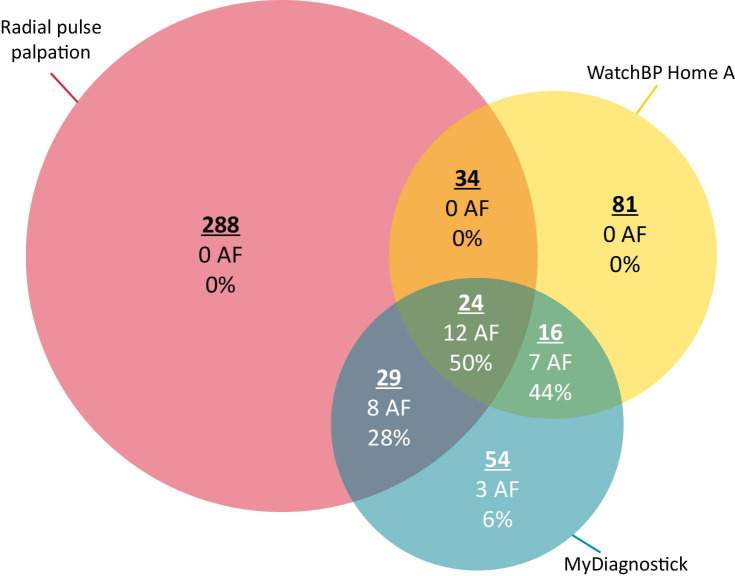
Results: We included 4339 patients; 0.8% showed new AF. Sensitivity and specificity were 62.8% (range 43.1%-69.7%) and 91.8% (91.7%-91.8%) for radial pulse palpation, 70.0% (49.0%-80.6%) and 96.5% (96.3%-96.7%) for electronic blood pressure measurement and 90.1% (60.8%-100%) and 97.9% (97.8%-97.9%) for handheld ECG, respectively. Positive predictive values were 5.8% (5.3%-6.1%), 13.8% (12.2%-14.8%) and 25.2% (24.2%-25.8%), respectively. All negative predictive values were ≥99.7%.
Conclusion: In detecting AF, electronic blood pressure measurement (WatchBP Home A), but especially handheld ECG (MyDiagnostick) showed better diagnostic accuracy than radial pulse palpation.
Trial registration number: Netherlands Trial Register No. NL4776 (old NTR4914).
Keywords: cardiology; pacing & electrophysiology; preventive medicine.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Opportunistic screening versus usual care for detection of atrial fibrillation in primary care: cluster randomised controlled trial.BMJ. 2020 Sep 16;370:m3208. doi: 10.1136/bmj.m3208. BMJ. 2020. PMID: 32938633 Free PMC article. Clinical Trial.
-
Detecting and Diagnosing Atrial Fibrillation (D2AF): study protocol for a cluster randomised controlled trial.Trials. 2015 Oct 23;16:478. doi: 10.1186/s13063-015-1006-5. Trials. 2015. PMID: 26499449 Free PMC article. Clinical Trial.
-
Validity of daily self-pulse palpation for atrial fibrillation screening in patients 65 years and older: A cross-sectional study.PLoS Med. 2020 Mar 31;17(3):e1003063. doi: 10.1371/journal.pmed.1003063. eCollection 2020 Mar. PLoS Med. 2020. PMID: 32231369 Free PMC article.
-
Lead-I ECG for detecting atrial fibrillation in patients attending primary care with an irregular pulse using single-time point testing: A systematic review and economic evaluation.PLoS One. 2019 Dec 23;14(12):e0226671. doi: 10.1371/journal.pone.0226671. eCollection 2019. PLoS One. 2019. PMID: 31869370 Free PMC article.
-
Screening for atrial fibrillation with automated blood pressure measurement: Research evidence and practice recommendations.Int J Cardiol. 2016 Jan 15;203:465-73. doi: 10.1016/j.ijcard.2015.10.182. Epub 2015 Oct 26. Int J Cardiol. 2016. PMID: 26547741 Review.
Cited by
-
WATCH-PR: Comparison of the Pulse Rate of a WATCH-Type Blood Pressure Monitor with the Pulse Rate of a Conventional Ambulatory Blood Pressure Monitor.Bioengineering (Basel). 2025 May 5;12(5):492. doi: 10.3390/bioengineering12050492. Bioengineering (Basel). 2025. PMID: 40428111 Free PMC article.
-
Smartphone and wearable detected atrial arrhythmias in Older Adults: Results of a fully digital European Case finding study.Eur Heart J Digit Health. 2022 Nov 1;3(4):610-625. doi: 10.1093/ehjdh/ztac067. eCollection 2022 Dec. Eur Heart J Digit Health. 2022. PMID: 36710894 Free PMC article.
-
Electrocardiogram Devices for Home Use: Technological and Clinical Scoping Review.JMIR Cardio. 2023 Jul 7;7:e44003. doi: 10.2196/44003. JMIR Cardio. 2023. PMID: 37418308 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical