

SARS-CoV-2 antibody trajectories after a single COVID-19 vaccination with and without prior infection
- PMID: 35768431
- PMCID: PMC9243074
- DOI: 10.1038/s41467-022-31495-x
SARS-CoV-2 antibody trajectories after a single COVID-19 vaccination with and without prior infection
Abstract
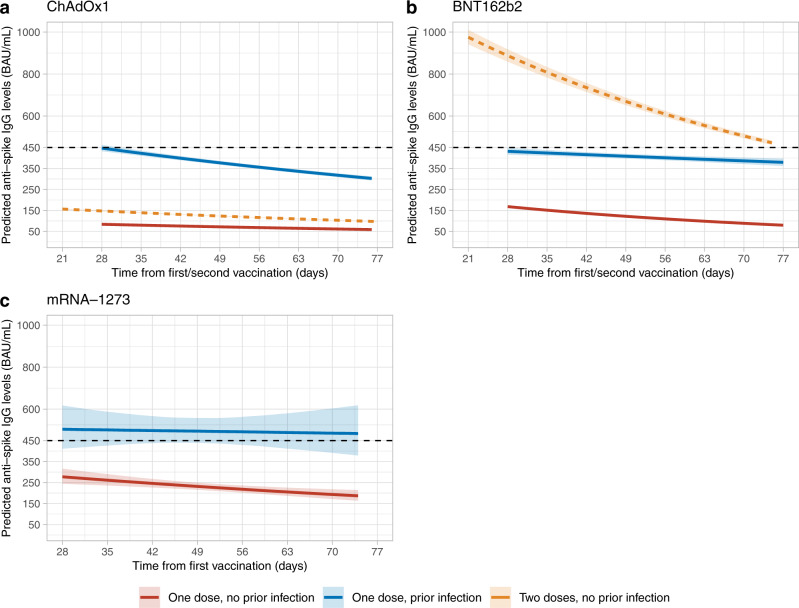
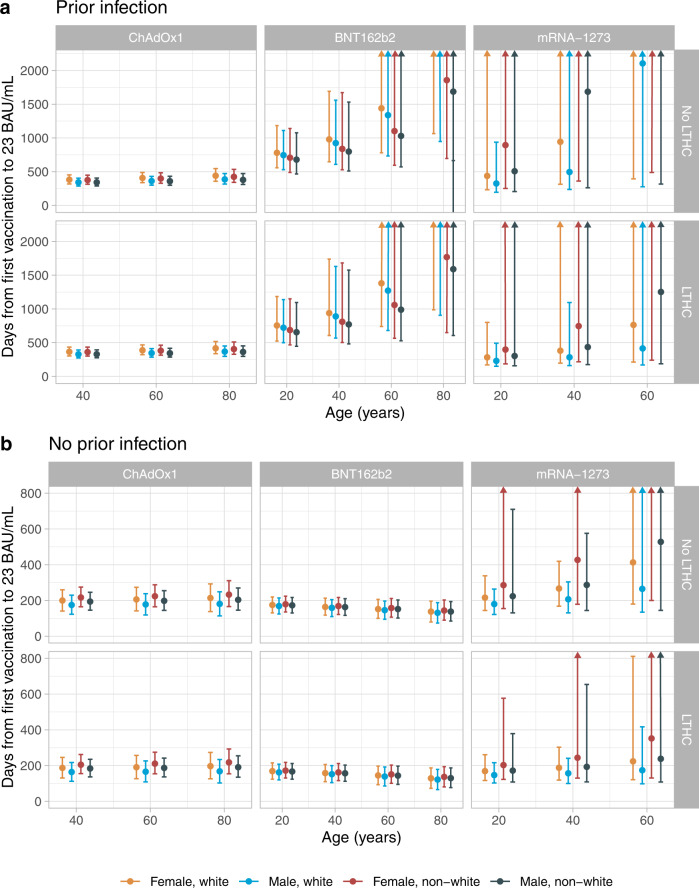
Given high SARS-CoV-2 incidence, coupled with slow and inequitable vaccine roll-out in many settings, there is a need for evidence to underpin optimum vaccine deployment, aiming to maximise global population immunity. We evaluate whether a single vaccination in individuals who have already been infected with SARS-CoV-2 generates similar initial and subsequent antibody responses to two vaccinations in those without prior infection. We compared anti-spike IgG antibody responses after a single vaccination with ChAdOx1, BNT162b2, or mRNA-1273 SARS-CoV-2 vaccines in the COVID-19 Infection Survey in the UK general population. In 100,849 adults median (50 (IQR: 37-63) years) receiving at least one vaccination, 13,404 (13.3%) had serological/PCR evidence of prior infection. Prior infection significantly boosted antibody responses, producing higher peak levels and/or longer half-lives after one dose of all three vaccines than those without prior infection receiving one or two vaccinations. In those with prior infection, the median time above the positivity threshold was >1 year after the first vaccination. Single-dose vaccination targeted to those previously infected may provide at least as good protection to two-dose vaccination among those without previous infection.
© 2022. The Author(s).
Conflict of interest statement
D.W.E. declares lecture fees from Gilead, outside the submitted work. No other author has a conflict of interest to declare.
Figures
References
-
- WHO Coronavirus (COVID-19) Dashboard WHO Coronavirus (COVID-19) Dashboard With Vaccination Data. 2022 https://covid19.who.int/?adgroupsurvey={adgroupsurvey}&gclid=CjwKCAjwopW....
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
