

International electronic health record-derived post-acute sequelae profiles of COVID-19 patients
- PMID: 35768548
- PMCID: PMC9242995
- DOI: 10.1038/s41746-022-00623-8
International electronic health record-derived post-acute sequelae profiles of COVID-19 patients
Abstract
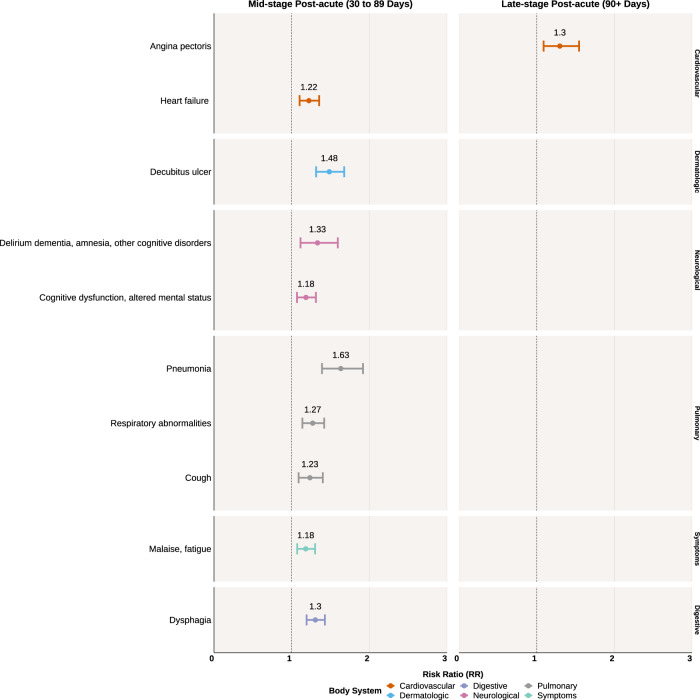
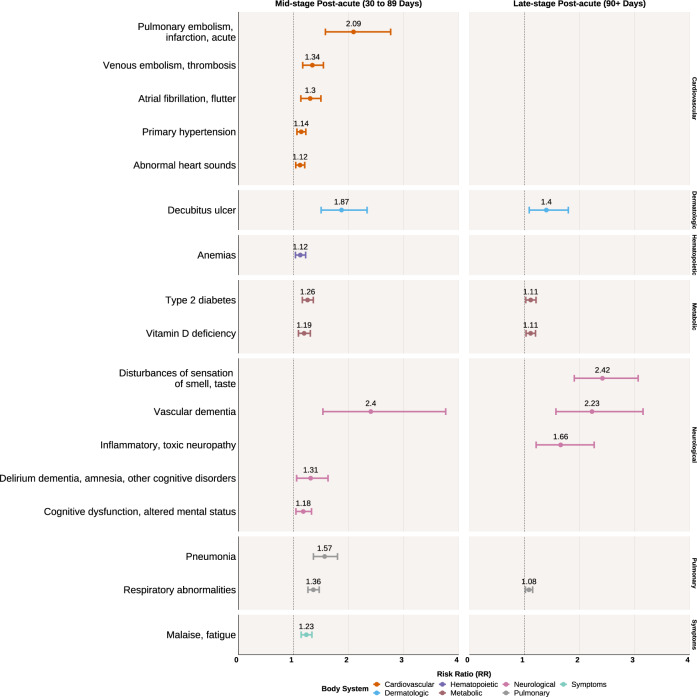
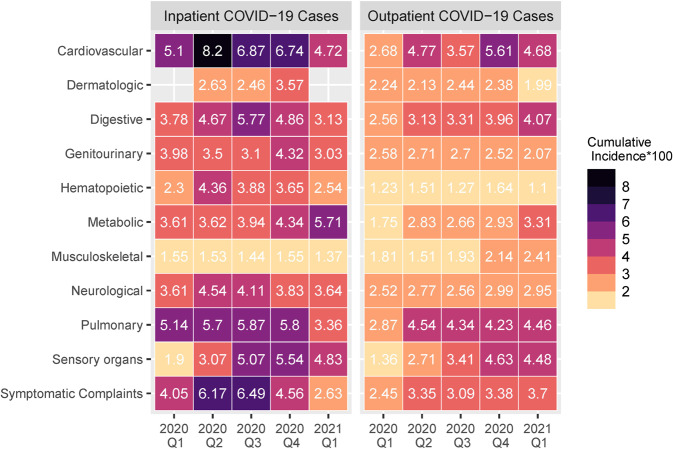
The risk profiles of post-acute sequelae of COVID-19 (PASC) have not been well characterized in multi-national settings with appropriate controls. We leveraged electronic health record (EHR) data from 277 international hospitals representing 414,602 patients with COVID-19, 2.3 million control patients without COVID-19 in the inpatient and outpatient settings, and over 221 million diagnosis codes to systematically identify new-onset conditions enriched among patients with COVID-19 during the post-acute period. Compared to inpatient controls, inpatient COVID-19 cases were at significant risk for angina pectoris (RR 1.30, 95% CI 1.09-1.55), heart failure (RR 1.22, 95% CI 1.10-1.35), cognitive dysfunctions (RR 1.18, 95% CI 1.07-1.31), and fatigue (RR 1.18, 95% CI 1.07-1.30). Relative to outpatient controls, outpatient COVID-19 cases were at risk for pulmonary embolism (RR 2.10, 95% CI 1.58-2.76), venous embolism (RR 1.34, 95% CI 1.17-1.54), atrial fibrillation (RR 1.30, 95% CI 1.13-1.50), type 2 diabetes (RR 1.26, 95% CI 1.16-1.36) and vitamin D deficiency (RR 1.19, 95% CI 1.09-1.30). Outpatient COVID-19 cases were also at risk for loss of smell and taste (RR 2.42, 95% CI 1.90-3.06), inflammatory neuropathy (RR 1.66, 95% CI 1.21-2.27), and cognitive dysfunction (RR 1.18, 95% CI 1.04-1.33). The incidence of post-acute cardiovascular and pulmonary conditions decreased across time among inpatient cases while the incidence of cardiovascular, digestive, and metabolic conditions increased among outpatient cases. Our study, based on a federated international network, systematically identified robust conditions associated with PASC compared to control groups, underscoring the multifaceted cardiovascular and neurological phenotype profiles of PASC.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Grants and funding
- UL1 TR000005/TR/NCATS NIH HHS/United States
- R01LM013345/U.S. Department of Health & Human Services | NIH | U.S. National Library of Medicine (NLM)
- K23HL148394/U.S. Department of Health & Human Services | NIH | National Heart, Lung, and Blood Institute (NHLBI)
- CTSA Award #UL1TR002366/U.S. Department of Health & Human Services | NIH | National Center for Advancing Translational Sciences (NCATS)
- R01 NS098023/NS/NINDS NIH HHS/United States
- R01 NS124882/NS/NINDS NIH HHS/United States
- UL1TR002240/U.S. Department of Health & Human Services | NIH | National Center for Advancing Translational Sciences (NCATS)
- P30ES017885/U.S. Department of Health & Human Services | National Institutes of Health (NIH)
- R01 HL151643-01/U.S. Department of Health & Human Services | NIH | National Heart, Lung, and Blood Institute (NHLBI)
- UL1TR001998/U.S. Department of Health & Human Services | NIH | National Center for Advancing Translational Sciences (NCATS)
- UL1 TR001420/TR/NCATS NIH HHS/United States
- UL1TR002541/U.S. Department of Health & Human Services | NIH | National Center for Advancing Translational Sciences (NCATS)
- UL1TR001881/U.S. Department of Health & Human Services | NIH | National Center for Advancing Translational Sciences (NCATS)
- UL1 TR001998/TR/NCATS NIH HHS/United States
- UL1 TR001881/TR/NCATS NIH HHS/United States
- UL1 TR001857/TR/NCATS NIH HHS/United States
- T15 LM007092/LM/NLM NIH HHS/United States
- U24 HL148865/HL/NHLBI NIH HHS/United States
- R01 HG009174/HG/NHGRI NIH HHS/United States
- U24 CA210967/CA/NCI NIH HHS/United States
- R01 LM013345/LM/NLM NIH HHS/United States
- UL1 TR002541/TR/NCATS NIH HHS/United States
- UL1TR001420/U.S. Department of Health & Human Services | NIH | National Center for Advancing Translational Sciences (NCATS)
- UL1TR000005/U.S. Department of Health & Human Services | NIH | National Center for Advancing Translational Sciences (NCATS)
- L40HL148910/U.S. Department of Health & Human Services | NIH | National Heart, Lung, and Blood Institute (NHLBI)
- R01 HL151643/HL/NHLBI NIH HHS/United States
- UL1TR001857/U.S. Department of Health & Human Services | NIH | National Center for Advancing Translational Sciences (NCATS)
- 3U01HG008685-05S2/U.S. Department of Health & Human Services | NIH | National Human Genome Research Institute (NHGRI)
- P30 ES017885/ES/NIEHS NIH HHS/United States
- R01 LM013337/LM/NLM NIH HHS/United States
- K23 HL148394/HL/NHLBI NIH HHS/United States
- UL1 TR002240/TR/NCATS NIH HHS/United States
- L40 HL148910/HL/NHLBI NIH HHS/United States
- U01 HG008685/HG/NHGRI NIH HHS/United States
- 5UL1TR001857-05/U.S. Department of Health & Human Services | NIH | National Center for Advancing Translational Sciences (NCATS)
- U24CA210967/U.S. Department of Health & Human Services | National Institutes of Health (NIH)
- 5R01HG009174-04/U.S. Department of Health & Human Services | NIH | National Human Genome Research Institute (NHGRI)
- UL1 TR002366/TR/NCATS NIH HHS/United States
- R01LM013337/U.S. Department of Health & Human Services | NIH | U.S. National Library of Medicine (NLM)
- R01NS098023/U.S. Department of Health & Human Services | NIH | National Institute of Neurological Disorders and Stroke (NINDS)
LinkOut - more resources
Full Text Sources
