

Rapid early progression (REP) of glioblastoma is an independent negative prognostic factor: Results from a systematic review and meta-analysis
- PMID: 35769410
- PMCID: PMC9234755
- DOI: 10.1093/noajnl/vdac075
Rapid early progression (REP) of glioblastoma is an independent negative prognostic factor: Results from a systematic review and meta-analysis
Erratum in
-
Erratum to: Rapid early progression (REP) of glioblastoma is an independent negative prognostic factor: Results from a systematic review and meta-analysis.Neurooncol Adv. 2022 Aug 9;4(1):vdac125. doi: 10.1093/noajnl/vdac125. eCollection 2022 Jan-Dec. Neurooncol Adv. 2022. PMID: 35958979 Free PMC article.
Abstract
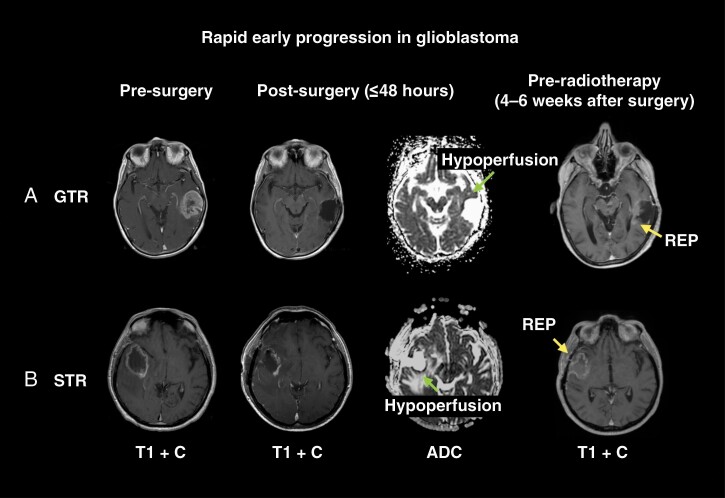
Background: In patients with newly diagnosed glioblastoma, rapid early progression (REP) refers to tumor regrowth between surgery and postoperative chemoradiotherapy. This systematic review and meta-analysis appraised previously published data on REP to better characterize and understand it.
Methods: Systematic searches of MEDLINE, EMBASE and the Cochrane database from inception to October 21, 2021. Studies describing the incidence of REP-tumor growth between the postoperative MRI scan and pre-radiotherapy MRI scan in newly diagnosed glioblastoma were included. The primary outcome was REP incidence.
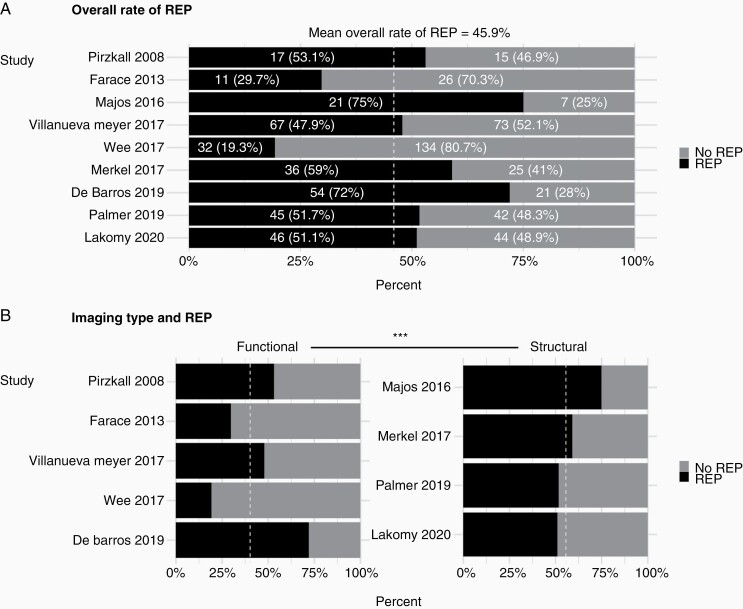
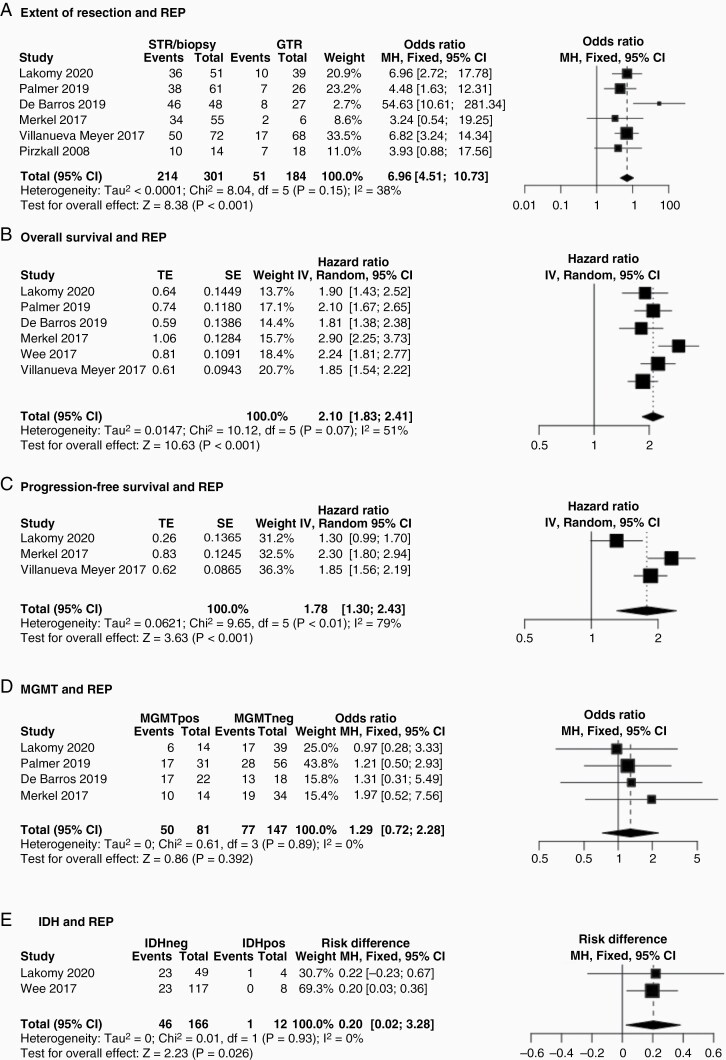
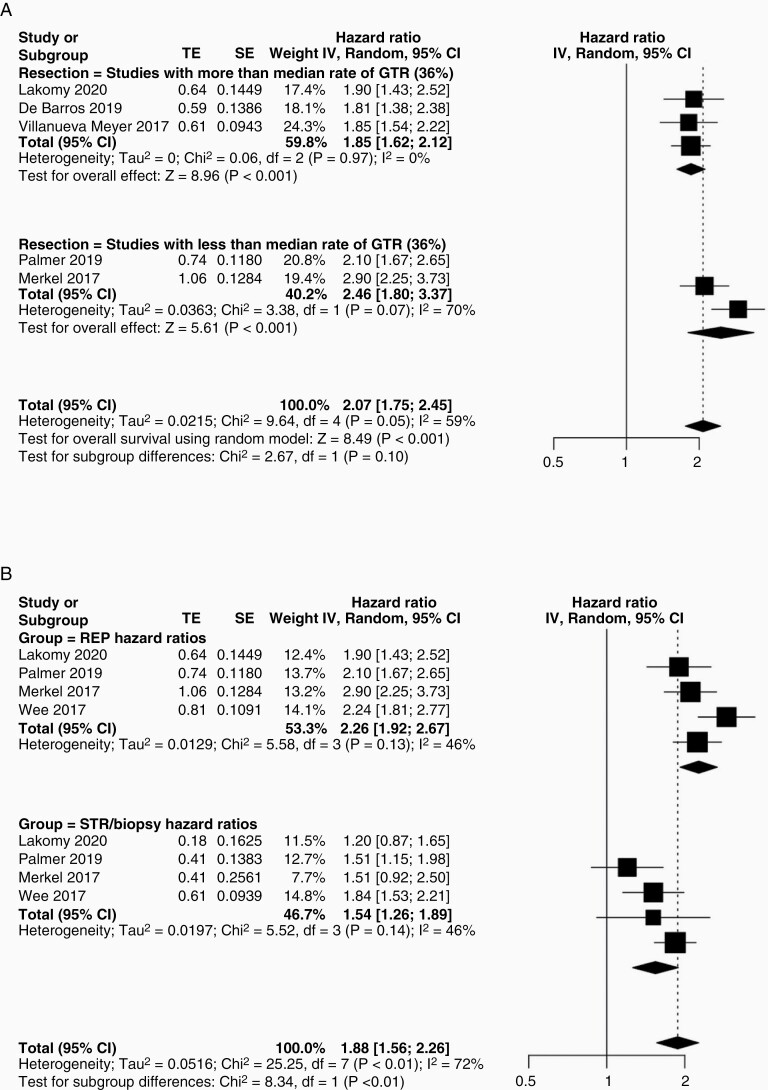
Results: From 1590 search results, 9 studies were included with 716 patients. The median age was 56.9 years (IQR 54.0-58.8 y). There was a male predominance with a median male-to-female ratio of 1.4 (IQR 1.1-1.5). The median number of days between MRI scans was 34 days (IQR 18-45 days). The mean incidence rate of REP was 45.9% (range 19.3%-72.0%) and significantly lower in studies employing functional imaging to define REP (P < .001). REP/non-REP groups were comparable with respect to age (P = .99), gender (P = .33) and time between scans (P = .81). REP was associated with shortened overall survival (HR 1.78, 95% CI 1.30-2.43, P < .001), shortened progression-free survival (HR 1.78, 95% CI 1.30-2.43, P < .001), subtotal resection (OR 6.96, 95% CI 4.51-10.73, P < .001) and IDH wild-type versus mutant tumors (OR 0.20, 95% CI 0.02-0.38, P = .03). MGMT promoter methylation was not associated with REP (OR 1.29, 95% CI 0.72-2.28, P = .39).
Conclusions: REP occurs in almost half of patients with newly diagnosed glioblastoma and has a strongly negative prognostic effect. Future studies should investigate its biology and effective treatment strategies.
Keywords: IDH; MGMT; REP; extent of resection; glioblastoma; prognosis; progression; recurrence; survival.
© The Author(s) 2022. Published by Oxford University Press, the Society for Neuro-Oncology and the European Association of Neuro-Oncology.
Figures
References
-
- Stupp R, Mason WP, van den Bent MJ, et al. . Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352(10):987–996. - PubMed
-
- Cantrell JN, Waddle MR, Rotman M, et al. . Progress toward long-term survivors of glioblastoma. Mayo Clin Proc. 2019;94(7):1278–1286. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials