

Reduced Opioid Use and Prescribing in a Same Day Discharge Pilot Enhanced Recovery Program for Elective Minimally Invasive Colorectal Surgical Procedures During the COVID-19 Pandemic
- PMID: 35771192
- PMCID: PMC9253719
- DOI: 10.1177/00031348221109467
Reduced Opioid Use and Prescribing in a Same Day Discharge Pilot Enhanced Recovery Program for Elective Minimally Invasive Colorectal Surgical Procedures During the COVID-19 Pandemic
Abstract
Purpose: Enhanced recovery pathways (ERPs) are associated with reduced complications and length of stay. The validation of the I-FEED scoring system, advances in perioperative anesthesia, multimodal analgesia, and telehealth remote monitoring have resulted in further evolution of ERPs setting the stage for same day discharge (SDD). Pioneers and early adopters have demonstrated the safety and feasibility of SDD programs. The aim of this study is to evaluate the impact of a pilot SDD ERP on patient self-reported pain scoring and narcotic usage.
Methods: A quality improvement pilot program was conducted to assess the impact of a SDD ERP on post-operative pain score reporting and opioid use in healthy patients undergoing elective colorectal surgery as an alternative to post-operative hospitalization during the COVID-19 pandemic (May 2020-December 2021). Patients were monitored remotely with daily telephone visits on POD 1-7 assessing the following variables: I-FEED score, pain score, pain management, bowel function, dietary advancement, any complications, and/or re-admissions.
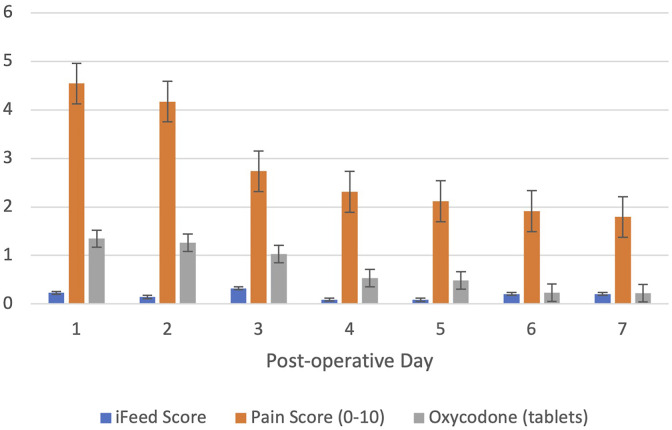
Results: Thirty-seven patients met the highly selective eligibility criteria for "healthy patient, healthy anastomosis." SDD occurred in 70%. The remaining 30% were discharged on POD 1. Mean total narcotic usage was 5.2 tablets of 5 mg oxycodone despite relatively high reported pain scores.
Conclusions: In our initial experience, SDD is associated with significantly lower patient narcotic utilization for postoperative pain management than hypothesized. This pilot SDD program resulted in a change in clinical practice with reduction of prescribed discharge oxycodone 5 mg quantity from #40 to #10 tablets.
Keywords: colectomy; colorectal surgery; enhanced recovery after surgery; enhanced recovery programs; home recovery; minimally invasive colectomy; multimodal analgesia; narcotic sparing; opioid prescribing and use; same day discharge.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures

References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
