Effect of Apatinib Plus Pegylated Liposomal Doxorubicin vs Pegylated Liposomal Doxorubicin Alone on Platinum-Resistant Recurrent Ovarian Cancer: The APPROVE Randomized Clinical Trial
- PMID: 35771546
- PMCID: PMC9247861
- DOI: 10.1001/jamaoncol.2022.2253
Effect of Apatinib Plus Pegylated Liposomal Doxorubicin vs Pegylated Liposomal Doxorubicin Alone on Platinum-Resistant Recurrent Ovarian Cancer: The APPROVE Randomized Clinical Trial
Abstract
Importance: There are substantial unmet therapeutic needs in patients with platinum-resistant recurrent ovarian cancer (PROC), and novel therapeutic strategies should be explored.
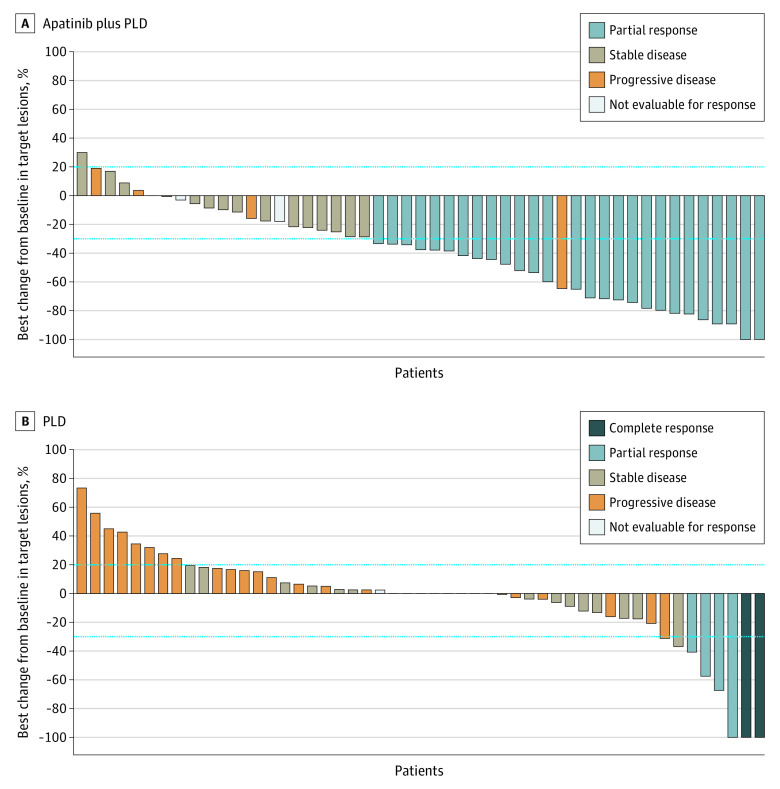
Objective: To evaluate the efficacy and safety of treatment with apatinib (a vascular endothelial growth factor receptor 2 tyrosine kinase inhibitor) plus pegylated liposomal doxorubicin (PLD) for PROC.
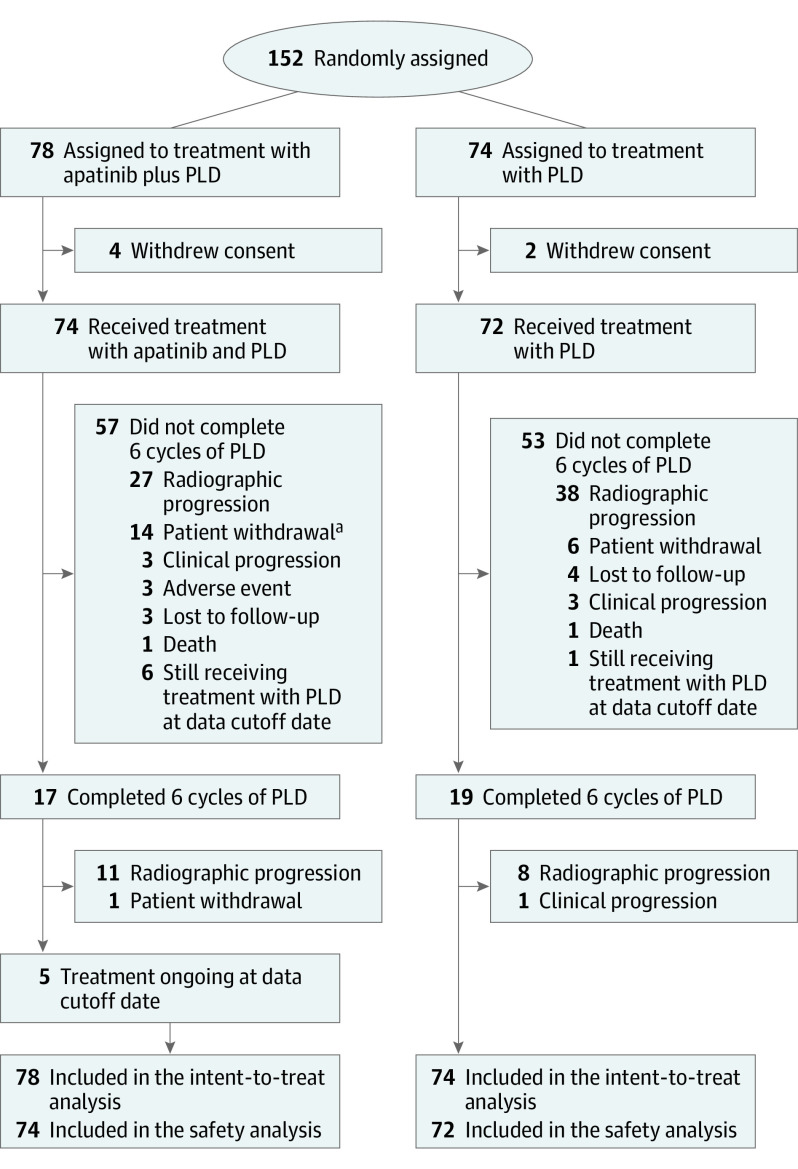
Design, setting, and participants: The APPROVE trial was performed as an open-label, randomized clinical trial at 11 hospitals in China between March 22, 2018, and November 16, 2020. Patients with histologically confirmed ovarian cancer who had experienced disease progression during or within 6 months of discontinuing any prior line of treatment with platinum-based chemotherapy were eligible. This primary analysis was based on data that were current as of January 28, 2021.
Interventions: Patients received PLD alone (40 mg/m2, intravenously, every 4 weeks, for up to 6 cycles) or PLD plus apatinib (250 mg, orally, daily).
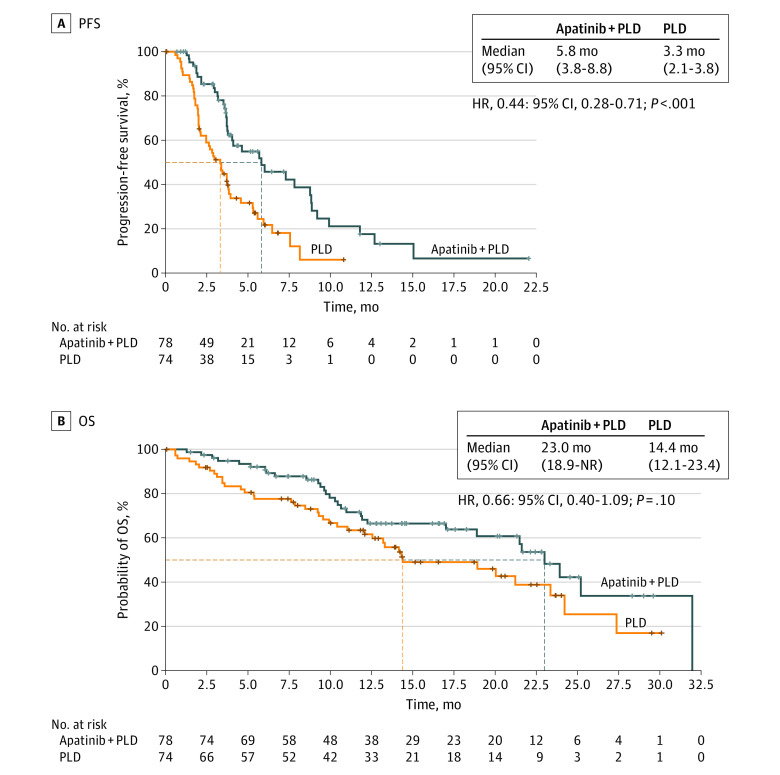
Main outcomes and measures: The primary end point was progression-free survival (PFS) by Response Evaluation Criteria in Solid Tumours (RECIST), version 1.1, in the intent-to-treat population.
Results: In total, 152 female patients were randomized, with 78 (51.3%) in the apatinib plus PLD group (median age, 54 years; range, 22-76 years) and 74 (48.7%) in the PLD group (median age, 56 years; range, 33-72 years). The median follow-up duration was 8.7 months (IQR, 4.7-14.1 months). The median PFS was 5.8 months (95% CI, 3.8-8.8) for treatment with apatinib plus PLD vs 3.3 months (95% CI, 2.1-3.8) for PLD (hazard ratio, 0.44; 95% CI, 0.28-0.71; P < .001). The median overall survival was 23.0 months (95% CI, 18.9 to not reached) with treatment with apatinib plus PLD vs 14.4 months (95% CI, 12.1-23.4) with PLD (hazard ratio, 0.66; 95% CI, 0.40-1.09). The most frequent grade 3 or higher treatment-emergent adverse events were decreased neutrophil counts (11 [14.9%] in the apatinib plus PLD group vs 6 [8.3%] in the PLD group), hypertension (6 [8.1%] vs none), and decreased white blood cell count (5 [6.8%] vs 3 [4.2%]). Two patients receiving treatment with apatinib plus PLD experienced grade 2 fistulas.
Conclusions and relevance: This randomized clinical trial found that treatment with apatinib plus PLD showed promising efficacy and manageable toxic effects in patients with PROC and may be a new alternative treatment option in this setting.
Trial registration: Clinicaltrials.gov Identifier: NCT04348032.
Conflict of interest statement
Figures