

A Phase 3, Open-Label Study of Lumacaftor/Ivacaftor in Children 1 to Less Than 2 Years of Age with Cystic Fibrosis Homozygous for F508del-CFTR
- PMID: 35771568
- PMCID: PMC9746849
- DOI: 10.1164/rccm.202204-0734OC
A Phase 3, Open-Label Study of Lumacaftor/Ivacaftor in Children 1 to Less Than 2 Years of Age with Cystic Fibrosis Homozygous for F508del-CFTR
Abstract
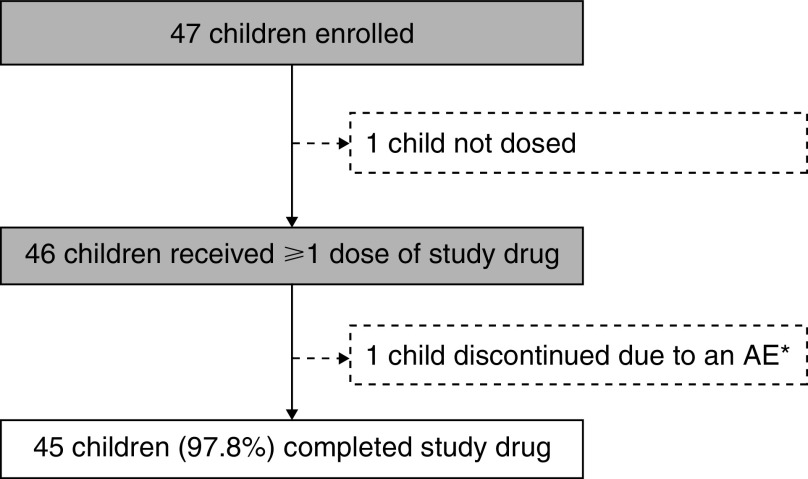
Rationale: Previous phase 3 trials showed that treatment with lumacaftor/ivacaftor was safe and efficacious in people aged ⩾2 years with cystic fibrosis (CF) homozygous for the F508del mutation in CFTR (CF transmembrane conductance regulator) (F/F genotype). Objectives: To assess the safety, pharmacokinetics, and pharmacodynamics of lumacaftor/ivacaftor in children aged 1 to <2 years with the F/F genotype. Methods: This open-label, phase 3 study consisted of two parts (part A [n = 14] and part B [n = 46]) in which two cohorts were enrolled on the basis of age (cohort 1, 18 to <24 mo; cohort 2, 12 to <18 mo). For the 15-day treatment period in part A, the lumacaftor/ivacaftor dose was based on weight at screening. Pharmacokinetic data from part A were used to determine dose-based weight boundaries for part B (24-wk treatment period). Measurements and Main Results: The primary endpoint of part A was pharmacokinetics, and the primary endpoint for part B was safety and tolerability. Secondary endpoints for part B were absolute change in sweat chloride concentration from baseline at Week 24 and pharmacokinetics. Analysis of pharmacokinetic data from part A confirmed the appropriateness of part B dosing. In part B, 44 children (95.7%) had adverse events, which for most were either mild (52.2% of children) or moderate (39.1% of children) in severity. The most common adverse events were cough, infective pulmonary exacerbation of CF, pyrexia, and vomiting. At Week 24, mean absolute change from baseline in sweat chloride concentration was -29.1 mmol/L (95% confidence interval, -34.8 to -23.4 mmol/L). Growth parameters (body mass index, weight, length, and associated z-scores) were normal at baseline and remained normal during the 24-week treatment period. Improving trends in some biomarkers of pancreatic function and intestinal inflammation, such as fecal elastase-1, serum immunoreactive trypsinogen, and fecal calprotectin, were observed. Conclusions: Lumacaftor/ivacaftor was generally safe and well tolerated in children aged 1 to <2 years with the F/F genotype, with a pharmacokinetic profile consistent with studies in older children. Efficacy results, including robust reductions in sweat chloride concentration, suggest the potential for CF disease modification with lumacaftor/ivacaftor treatment. These results support the use of lumacaftor/ivacaftor in this population. Clinical trial registered with www.clinicaltrials.gov (NCT03601637).
Keywords: children; cystic fibrosis; ivacaftor; lumacaftor.
Figures



Comment in
-
A New Era for Cystic Fibrosis and Cystic Fibrosis Transmembrane Conductance Regulator Modulator Trials in Infants.Am J Respir Crit Care Med. 2022 Nov 15;206(10):1193-1195. doi: 10.1164/rccm.202207-1356ED. Am J Respir Crit Care Med. 2022. PMID: 35856818 Free PMC article. No abstract available.
References
-
- Elborn JS. Cystic fibrosis. Lancet . 2016;388:2519–2531. - PubMed
-
- Riordan JR, Rommens JM, Kerem B, Alon N, Rozmahel R, Grzelczak Z, et al. Identification of the cystic fibrosis gene: cloning and characterization of complementary DNA. Science . 1989;245:1066–1073. - PubMed
-
- Anderson MP, Gregory RJ, Thompson S, Souza DW, Paul S, Mulligan RC, et al. Demonstration that CFTR is a chloride channel by alteration of its anion selectivity. Science . 1991;253:202–205. - PubMed
-
- VanDevanter DR, Kahle JS, O’Sullivan AK, Sikirica S, Hodgkins PS. Cystic fibrosis in young children: A review of disease manifestation, progression, and response to early treatment. J Cyst Fibros . 2016;15:147–157. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
