

Accelerating 3D MTC-BOOST in patients with congenital heart disease using a joint multi-scale variational neural network reconstruction
- PMID: 35772584
- PMCID: PMC9826869
- DOI: 10.1016/j.mri.2022.06.012
Accelerating 3D MTC-BOOST in patients with congenital heart disease using a joint multi-scale variational neural network reconstruction
Abstract
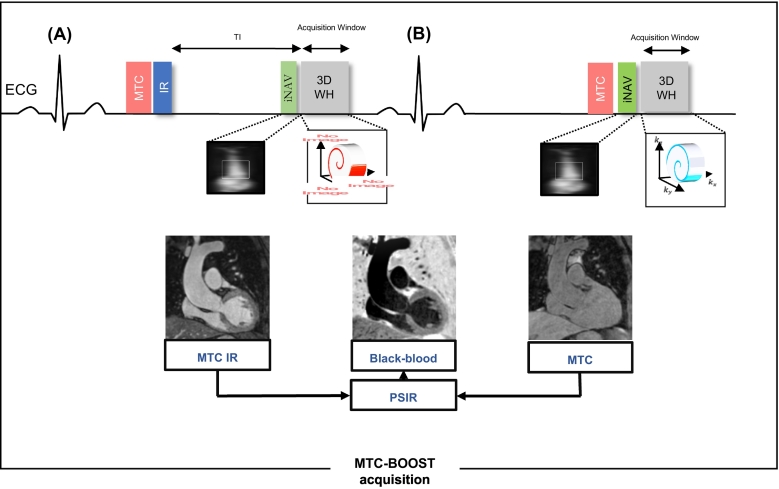
Purpose: Free-breathing Magnetization Transfer Contrast Bright blOOd phase SensiTive (MTC-BOOST) is a prototype balanced-Steady-State Free Precession sequence for 3D whole-heart imaging, that employs the endogenous magnetisation transfer contrast mechanism. This achieves reduction of flow and off-resonance artefacts, that often arise with the clinical T2prepared balanced-Steady-State Free Precession sequence, enabling high quality, contrast-agent free imaging of the thoracic cardiovascular anatomy. Fully-sampled MTC-BOOST acquisition requires long scan times (~10-24 min) and therefore acceleration is needed to permit its clinical incorporation. The aim of this study is to enable and clinically validate the 5-fold accelerated MTC-BOOST acquisition with joint Multi-Scale Variational Neural Network (jMS-VNN) reconstruction.
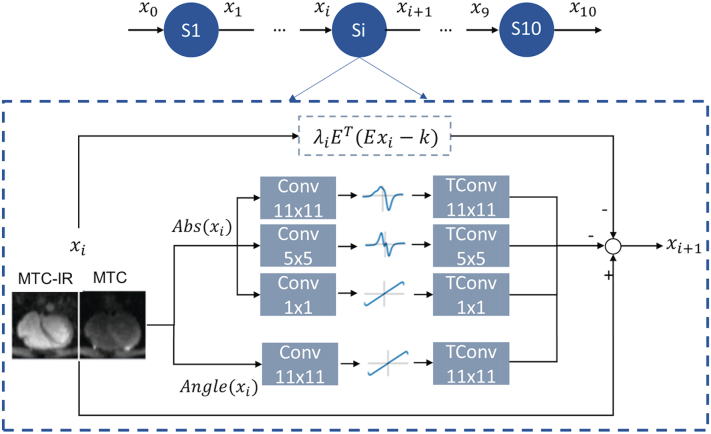
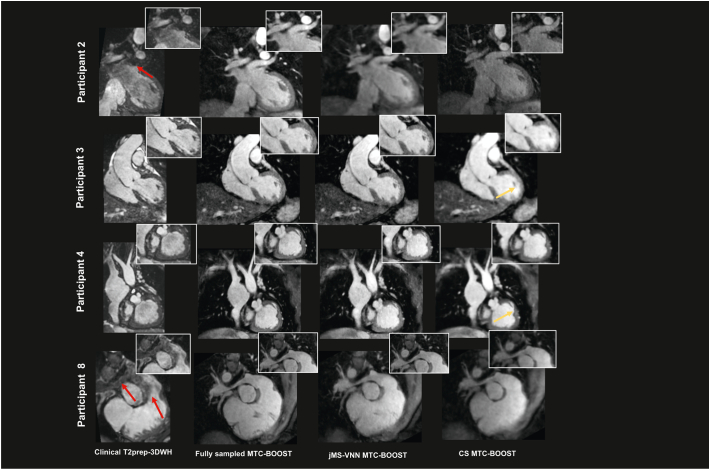
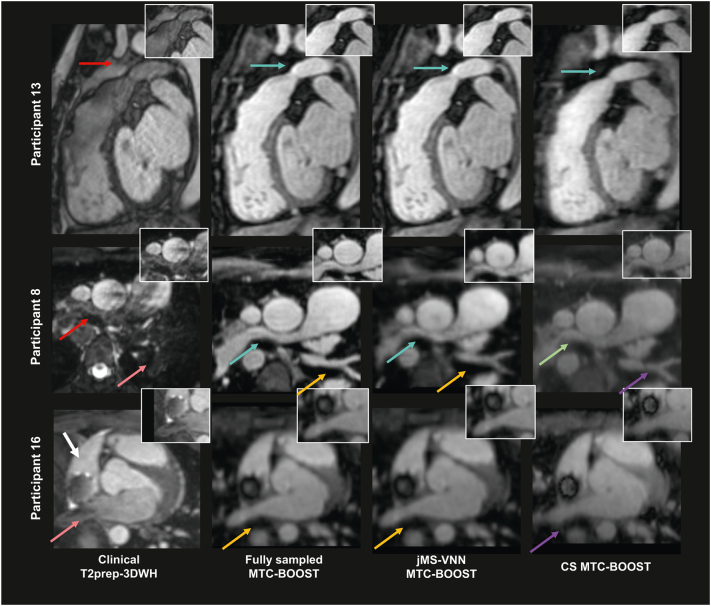
Methods: Thirty-six patients underwent free-breathing, 3D whole-heart imaging with the MTC-BOOST sequence, which is combined with variable density spiral-like Cartesian sampling and 2D image navigators for translational motion estimation. This sequence acquires two differently weighted bright-blood volumes in an interleaved fashion, which are then joined in a phase sensitive inversion recovery reconstruction to obtain a complementary fully co-registered black-blood volume. Data from eighteen patients were used for training, whereas data from the remaining eighteen patients were used for testing/evaluation. The proposed deep-learning based approach adopts a supervised multi-scale variational neural network for joint reconstruction of the two differently weighted bright-blood volumes acquired with the 5-fold accelerated MTC-BOOST. The two contrast images are stacked as different channels in the network to exploit the shared information. The proposed approach is compared to the fully-sampled MTC-BOOST and 5-fold undersampled MTC-BOOST acquisition with Compressed Sensing (CS) reconstruction in terms of scan/reconstruction time and bright-blood image quality. Comparison against conventional 2-fold undersampled T2-prepared 3D bright-blood whole-heart clinical sequence (T2prep-3DWH) is also included.
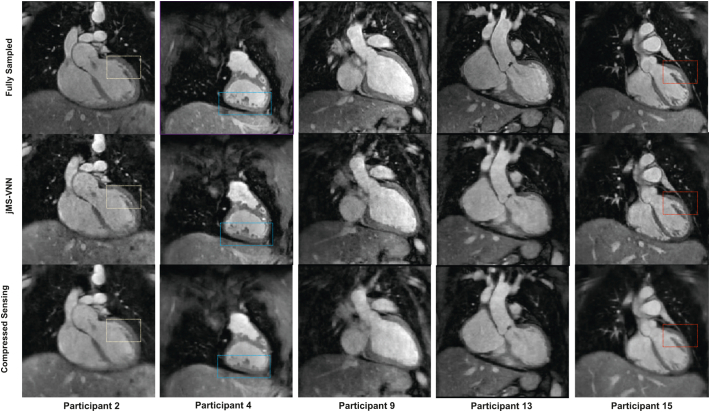
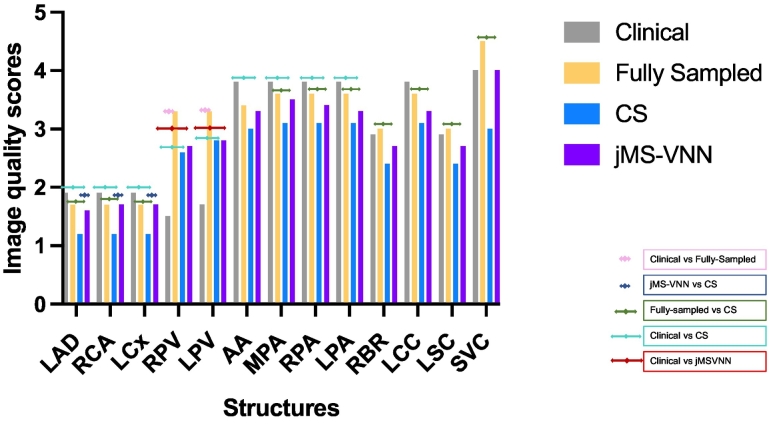
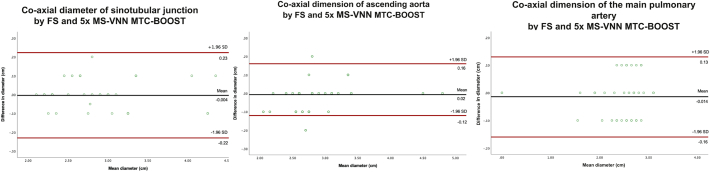
Results: Acquisition time was 3.0 ± 1.0 min for the 5-fold accelerated MTC-BOOST versus 9.0 ± 1.1 min for the fully-sampled MTC-BOOST and 11.1 ± 2.6 min for the T2prep-3DWH (p < 0.001 and p < 0.001, respectively). Reconstruction time was significantly lower with the jMS-VNN method compared to CS (10 ± 0.5 min vs 20 ± 2 s, p < 0.001). Image quality was higher for the proposed 5-fold undersampled jMS-VNN versus conventional CS, comparable or higher to the corresponding T2prep-3DWH dataset and similar to the fully-sampled MTC-BOOST.
Conclusion: The proposed 5-fold accelerated jMS-VNN MTC-BOOST framework provides efficient 3D whole-heart bright-blood imaging in fast acquisition and reconstruction time with concomitant reduction of flow and off-resonance artefacts, that are frequently encountered with the clinical sequence. Image quality of the cardiac anatomy and thoracic vasculature is comparable or superior to the clinical scan and 5-fold CS reconstruction in faster reconstruction time, promising potential clinical adoption.
Keywords: 3D whole-heart imaging; Cardiac MRI; Free-breathing; Neural network.
Copyright © 2022 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
All the authors declare that they do not have competing interests.
Figures
References
-
- Buber J., Valente A.M. Predicting survival in adults with congenital heart disease: what are the odds? Heart (British Cardiac Society) 2018;104(20):1643–1644. - PubMed
-
- Fratz S., Chung T., Greil G.F., et al. Guidelines and protocols for cardiovascular magnetic resonance in children and adults with congenital heart disease: SCMR expert consensus group on congenital heart disease. J Cardiovasc Magn Reson. 2013;15(1):51. doi: 10.1186/1532-429X-15-51. - DOI - PMC - PubMed
-
- Sorensen T.S., Korperich H., Greil G.F., et al. Operator-independent isotropic three-dimensional magnetic resonance imaging for morphology in congenital heart disease: a validation study. Circulation. 2004;110(2):163–169. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
