

Treatment of Odontoid Fractures in Elderly Patients Using C1/C2 Instrumented Fusion Supplemented With Bilateral Atlantoaxial Joint Spacers: A Case Series
- PMID: 35772974
- PMCID: PMC9650199
- DOI: 10.14444/8250
Treatment of Odontoid Fractures in Elderly Patients Using C1/C2 Instrumented Fusion Supplemented With Bilateral Atlantoaxial Joint Spacers: A Case Series
Abstract
Background: Spinal fractures are among the most common traumatic injuries in elderly patients, with the odontoid process being frequently affected. As this patient group usually has high rates of comorbidity and chronic diseases, a nonoperative approach may offer a reasonable solution for a favorable fracture pattern.
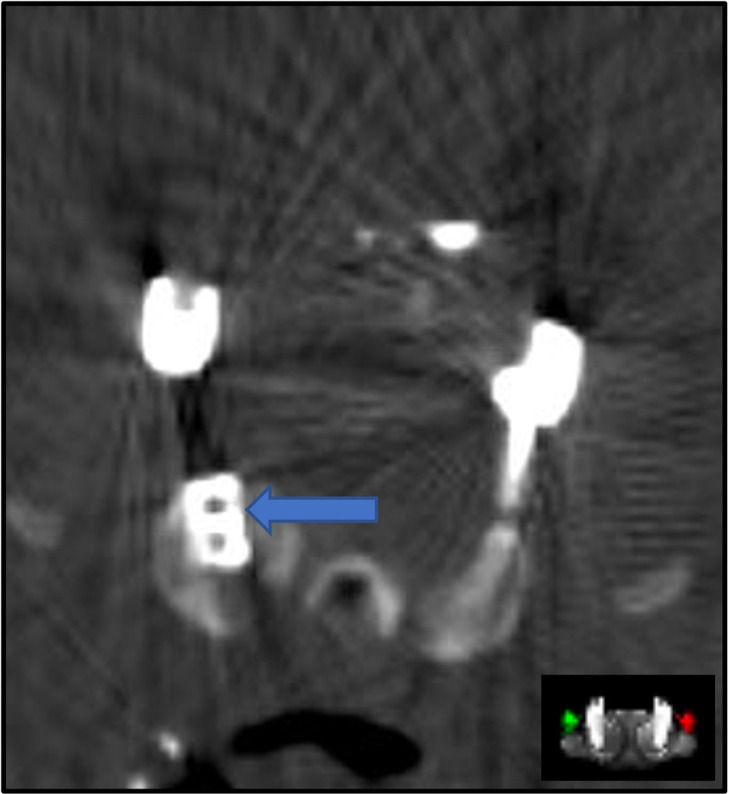
Objective: We modified the procedure by implanting a bilateral atlantoaxial joint spacer (model DTRAX) into the joint space and review our experience utilizing this technique for the treatment of patients with a fracture of the odontoid process.
Methods: A retrospective evaluation was performed on patients treated surgically for unstable traumatic fractures of the odontoid process. The stabilization was performed using a dorsal rod and screw instrumentation of the lateral mass of the atlas and the pars interarticularis of the axis. The procedure was further modified by implanting a bilateral atlantoaxial joint spacer (DTRAX) into the joint space bilaterally after the removal of the articular cartilage. Patients older than 70 years with a traumatic fracture of the odontoid process were included. Pain was assessed pre- and postoperatively using the visual analog scale (VAS). To verify fusion during follow-up, either x-ray imaging of the cervical spine or magnetic resonance imaging or computed tomography were performed.
Results: A total of 5 patients were included in our study. Four patients had an American Society of Anesthesiology score of 3 and 1 had a score of 4. The average duration of surgery was 187 ± 38.1 minutes. The average blood loss during the procedure was 340 ± 270 mL. The average radiological follow-up period was 21.2 ± 17.5 months. Preoperatively, the average VAS pain score was 2.3 ± 3.3. Postoperatively, the mean VAS decreased to 0.6 ± 0.9. The average follow-up period for pain was 27.2 ± 19 months. No patient showed neurological deficits before or after surgery. Follow-up demonstrated solid fusion in all cases.
Conclusion: The fusion of the atlantoaxial joint with bilateral atlantoaxial joint spacers represents a suitable and feasible option for achieving high fusion rates in elderly patients with odontoid fractures.
Clinical relevance: A significant percentage of patients who are treated non-operatively will experience nonunion, which may cause instability of the atlantoaxial joint. Posterior fixation with screws and rods is a treatment option, but it leaves the cartilaginous joint surface in place, which can be an impediment to the fusion process. In other cases, degenerative collapse of the C1/C2 joint can cause compression of the C2 nerve root.
Keywords: DTRAX; atlantoaxial fusion; cage implantation; cervical fusion; elderly; facet cages; geriatric patients; odontoid fracture; odontoid non union; odontoid pseudarthrosis.
This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
Conflict of interest statement
Declaration of Conflicting Interests: The authors report no conflicts of interest in this work.
Figures





References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous