

Different bimodal neuromodulation settings reduce tinnitus symptoms in a large randomized trial
- PMID: 35773272
- PMCID: PMC9246951
- DOI: 10.1038/s41598-022-13875-x
Different bimodal neuromodulation settings reduce tinnitus symptoms in a large randomized trial
Erratum in
-
Author Correction: Different bimodal neuromodulation settings reduce tinnitus symptoms in a large randomized trial.Sci Rep. 2023 Jul 10;13(1):11152. doi: 10.1038/s41598-023-38312-5. Sci Rep. 2023. PMID: 37430102 Free PMC article. No abstract available.
Abstract
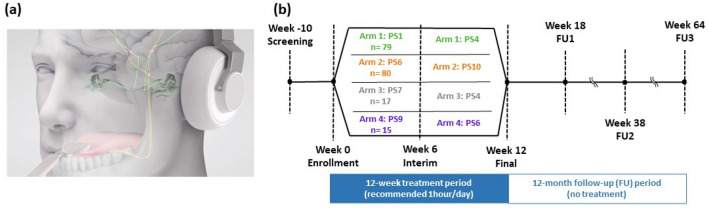
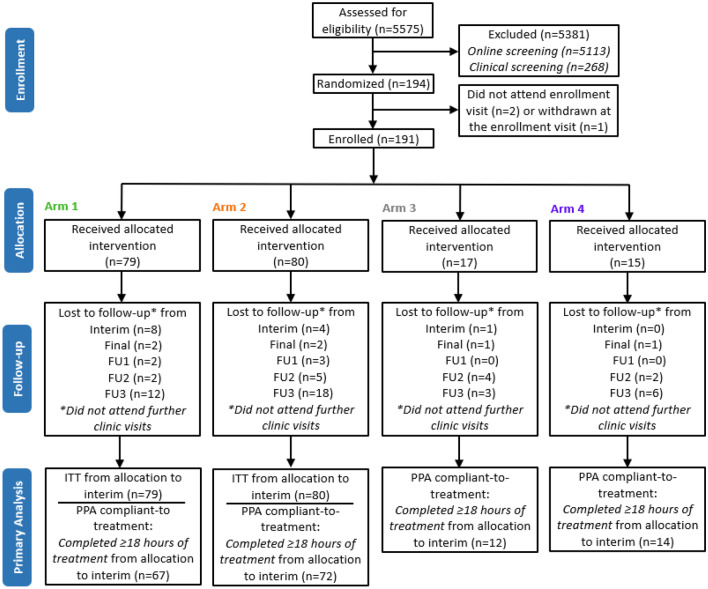
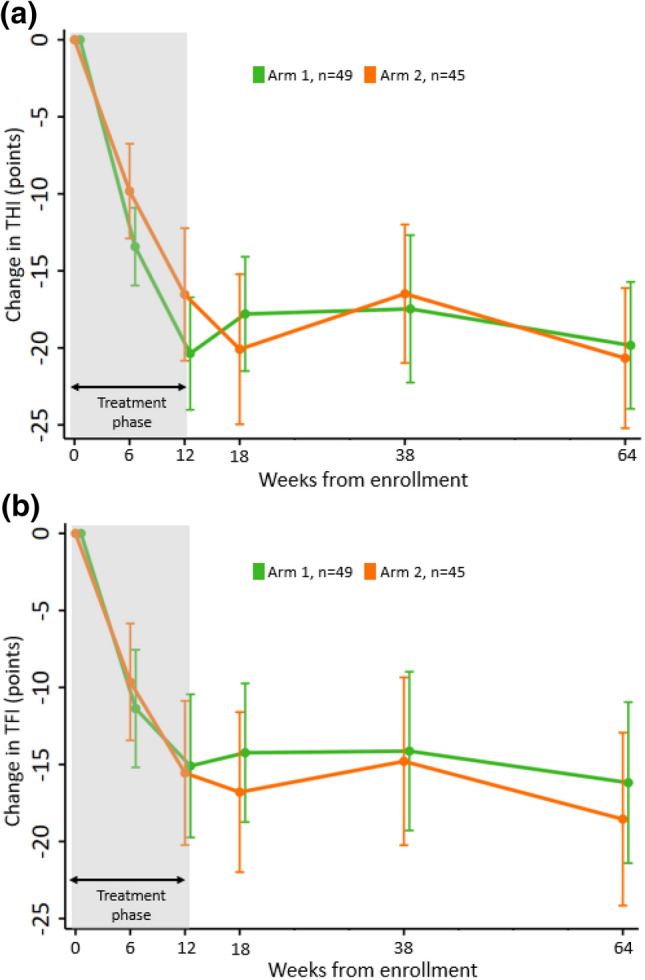
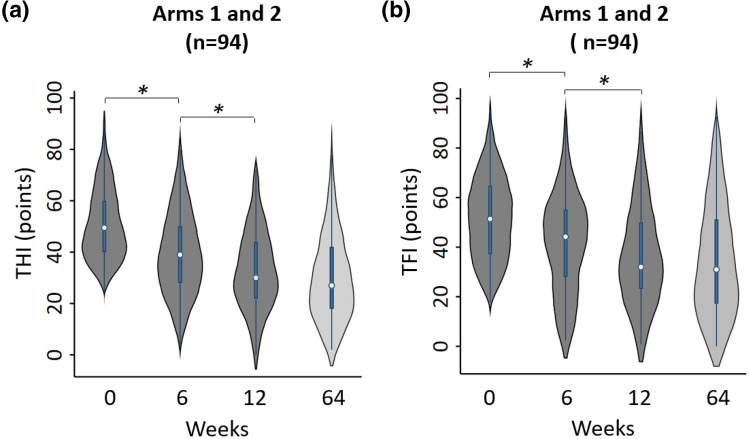
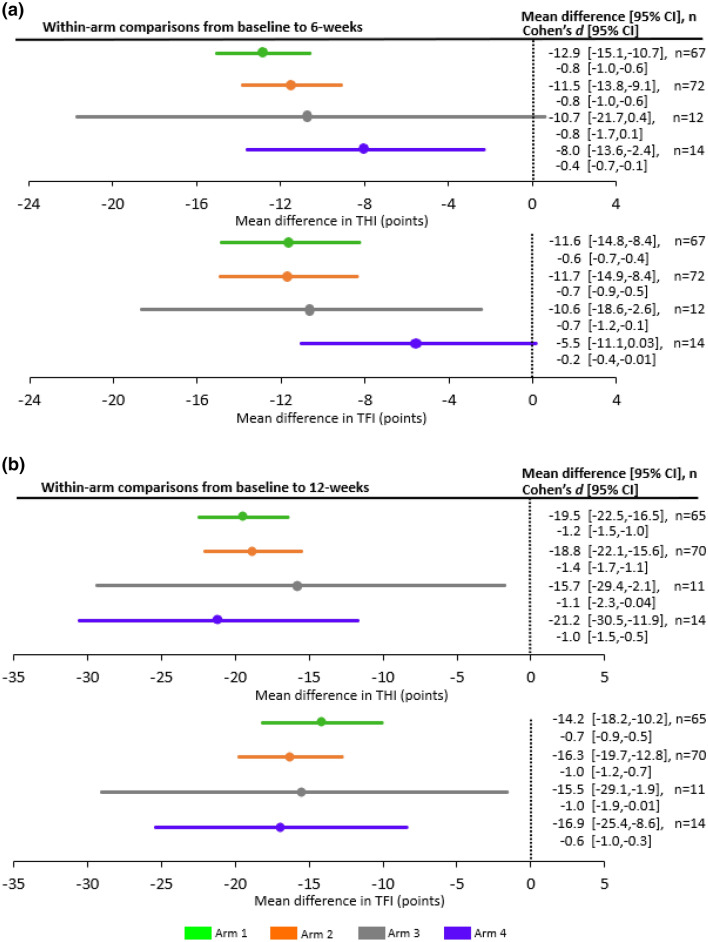
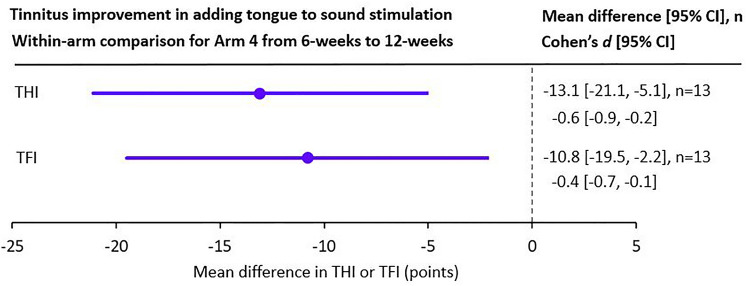
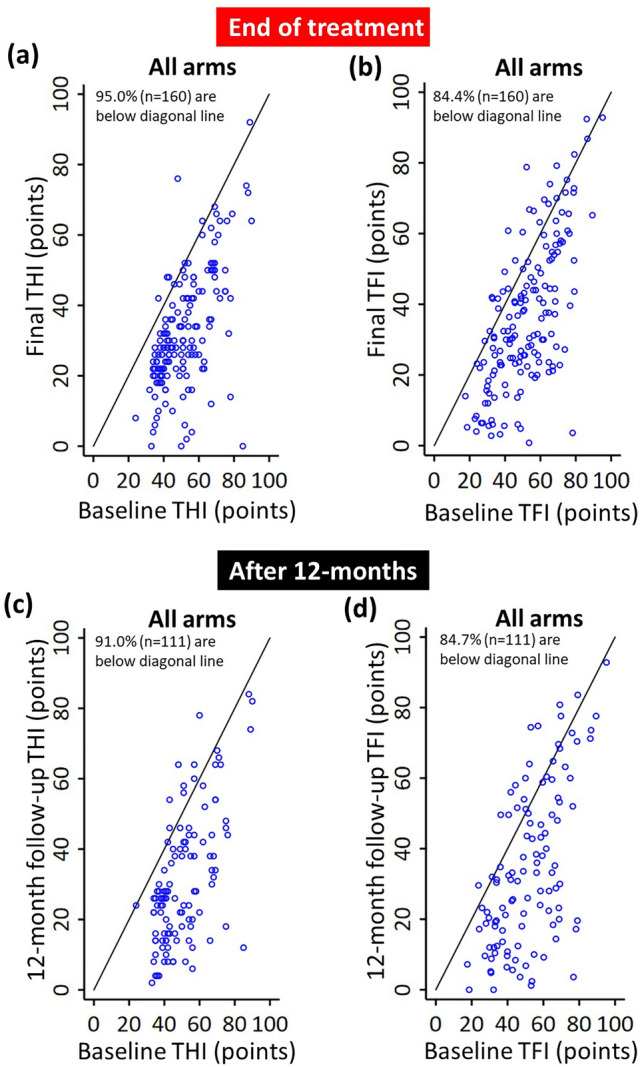
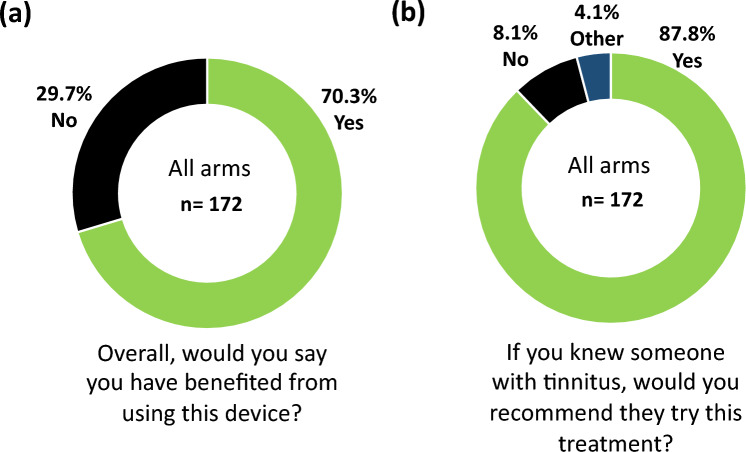
More than 10% of the population suffers from tinnitus, which is a phantom auditory condition that is coded within the brain. A new neuromodulation approach to treat tinnitus has emerged that combines sound with electrical stimulation of somatosensory pathways, supported by multiple animal studies demonstrating that bimodal stimulation can elicit extensive neural plasticity within the auditory brain. More recently, in a large-scale clinical trial, bimodal neuromodulation combining sound and tongue stimulation drove significant reductions in tinnitus symptom severity during the first 6 weeks of treatment, followed by diminishing improvements during the second 6 weeks of treatment. The primary objective of the large-scale randomized and double-blinded study presented in this paper was to determine if background wideband noise as used in the previous clinical trial was necessary for bimodal treatment efficacy. An additional objective was to determine if adjusting the parameter settings after 6 weeks of treatment could overcome treatment habituation effects observed in the previous study. The primary endpoint at 6-weeks involved within-arm and between-arm comparisons for two treatment arms with different bimodal neuromodulation settings based on two widely used and validated outcome instruments, Tinnitus Handicap Inventory and Tinnitus Functional Index. Both treatment arms exhibited a statistically significant reduction in tinnitus symptoms during the first 6-weeks, which was further reduced significantly during the second 6-weeks by changing the parameter settings (Cohen's d effect size for full treatment period per arm and outcome measure ranged from - 0.7 to - 1.4). There were no significant differences between arms, in which tongue stimulation combined with only pure tones and without background wideband noise was sufficient to reduce tinnitus symptoms. These therapeutic effects were sustained up to 12 months after the treatment ended. The study included two additional exploratory arms, including one arm that presented only sound stimuli during the first 6 weeks of treatment and bimodal stimulation in the second 6 weeks of treatment. This arm revealed the criticality of combining tongue stimulation with sound for treatment efficacy. Overall, there were no treatment-related serious adverse events and a high compliance rate (83.8%) with 70.3% of participants indicating benefit. The discovery that adjusting stimulation parameters overcomes previously observed treatment habituation can be used to drive greater therapeutic effects and opens up new opportunities for optimizing stimuli and enhancing clinical outcomes for tinnitus patients with bimodal neuromodulation.
© 2022. The Author(s).
Conflict of interest statement
Several of the authors have competing interests. BC, CH, EM, SLL, COC, SH, HHL are employees, consultants and/or shareholders of Neuromod Devices. BL, SV, DAH serve on the clinical advisory board of Neuromod Devices and receive monetary compensation for their contribution.
Figures
References
-
- Moller, A. R., Langguth, B., De Ridder, D. & Kleinjung, T. Textbook of Tinnitus 1–816 (Springer Science & Business Media, LLC New York, 2011).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
