

Cough hypersensitivity and chronic cough
- PMID: 35773287
- PMCID: PMC9244241
- DOI: 10.1038/s41572-022-00370-w
Cough hypersensitivity and chronic cough
Abstract
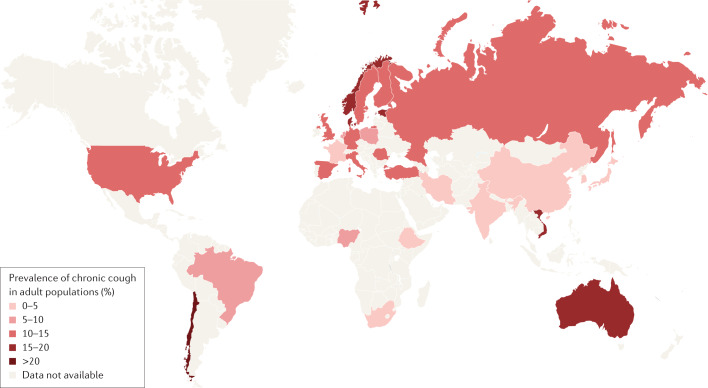
Chronic cough is globally prevalent across all age groups. This disorder is challenging to treat because many pulmonary and extrapulmonary conditions can present with chronic cough, and cough can also be present without any identifiable underlying cause or be refractory to therapies that improve associated conditions. Most patients with chronic cough have cough hypersensitivity, which is characterized by increased neural responsivity to a range of stimuli that affect the airways and lungs, and other tissues innervated by common nerve supplies. Cough hypersensitivity presents as excessive coughing often in response to relatively innocuous stimuli, causing significant psychophysical morbidity and affecting patients' quality of life. Understanding of the mechanisms that contribute to cough hypersensitivity and excessive coughing in different patient populations and across the lifespan is advancing and has contributed to the development of new therapies for chronic cough in adults. Owing to differences in the pathology, the organs involved and individual patient factors, treatment of chronic cough is progressing towards a personalized approach, and, in the future, novel ways to endotype patients with cough may prove valuable in management.
© 2022. Springer Nature Limited.
Conflict of interest statement
K.F.C. has received honoraria for participating on Advisory Board meetings of GSK, AstraZeneca, Novartis, Merck, Nocion, Shionogi and Reckitt Benckiser and on the Scientific Advisory Board of the Clean Breathing Institute supported by GSK Health Care Consumer Products. He has also been remunerated for speaking engagements by AstraZeneca, Novartis and Merck. L.M. reports honoraria from Chiesi, GSK, Merck, NeRRe Therapeutics, and Shionogi Inc.; grant support from Merck; and other support from AstraZeneca, Boehringer Ingelheim, Chiesi and Reckitt Benckiser. W.-J.S. declares grants from Merck and AstraZeneca, consulting fees from Merck, AstraZeneca, Shionogi and GSK, and lecture fees from Merck, AstraZeneca, GSK and Novartis. A.B.C. reports fees to her institution as IDMC Member of an unlicensed vaccine (GSK), an unlicensed molecule for chronic cough (Merck), IDMC Member of an unlicensed monoclonal antibody (AstraZeneca) and personal fees from being an author of two Up-to-date chapters. K.L. has received honoraria from AstraZeneca, Chiesi, Circassia, Daiichi Sankyo (China), GSK, Merck, Shionogi Inc. and Novartis; grant and other support from AstraZeneca, Chiesi, Circassia, Daiichi Sankyo (China), GSK and Merck. B.J.C. has received honoraria from Merck, GSK, Nocion, Axalbion, Menlo and Attenua, and grant support from Site One and Merck. S.S.B. reports honoraria from Merck, Bellus Health, Bayer, Shionogi, NeRRe, Menlo, Boehringer Ingelheim and Reckitt Benckiser. J.A.S. is an inventor on a patent describing methods for detecting cough from sound recordings, licensed to Vitalograph Ltd. J.A.S. has received funding for consultancy and research funds from Afferent Pharmaceuticals, Merck Inc., Bayer, Bellus, GSK, Xention Ltd, Ario Pharma Ltd, Glenmark, Almirall, AstraZeneca, Axalbion, Patara, Verona Pharma, NeRRe Pharmaceuticals, Menlo Pharmaceuticals and Attenua Inc. S.B.M. declares honoraria from Merck, NeRRe Therapeutics, Reckitt Benckiser and Bellus Health and grant support from Merck and Bellus Health. None of the disclosed entities above had any involvement in the conceptualization, design, data collection, analysis, decision to publish or preparation of the manuscript.
Figures


References
-
- Cherry DK, Burt CW, Woodwell DA. National ambulatory medical care survey: 2001 summary. Adv. Data. 2003;337:1–44. - PubMed
-
- Morice AH, et al. ERS guidelines on the assessment of cough. Eur. Respir. J. 2007;29:1256–1276. - PubMed
-
- Chang AB, Glomb WB. Guidelines for evaluating chronic cough in pediatrics: ACCP evidence-based clinical practice guidelines. Chest. 2006;129:260s–283s. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
