

Risk of recurrence after local resection of T1 rectal cancer: a meta-analysis with meta-regression
- PMID: 35773606
- PMCID: PMC9652303
- DOI: 10.1007/s00464-022-09396-3
Risk of recurrence after local resection of T1 rectal cancer: a meta-analysis with meta-regression
Abstract
Background: T1 rectal cancer (RC) patients are increasingly being treated by local resection alone but uniform surveillance strategies thereafter are lacking. To determine whether different local resection techniques influence the risk of recurrence and cancer-related mortality, a meta-analysis was performed.
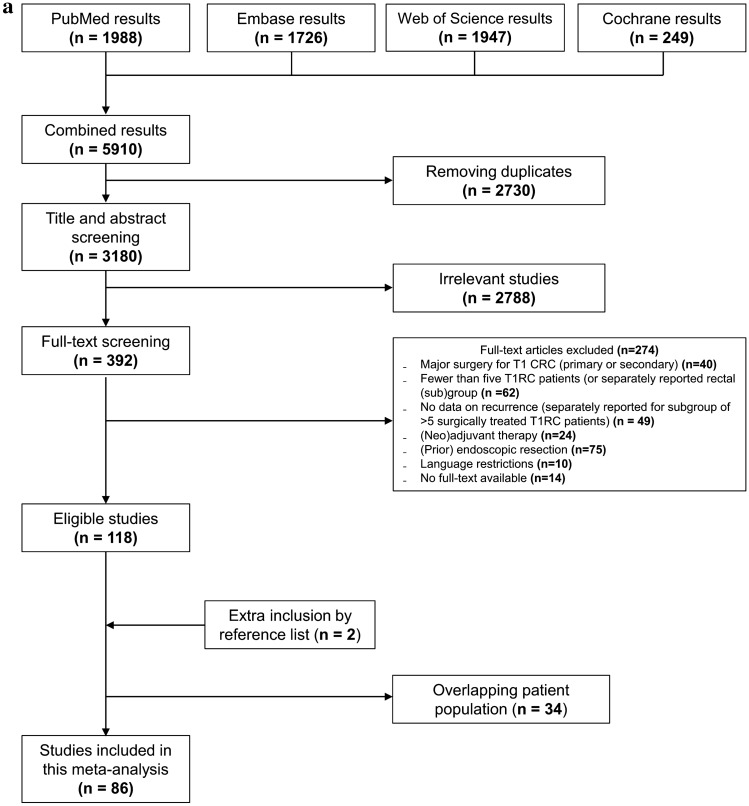
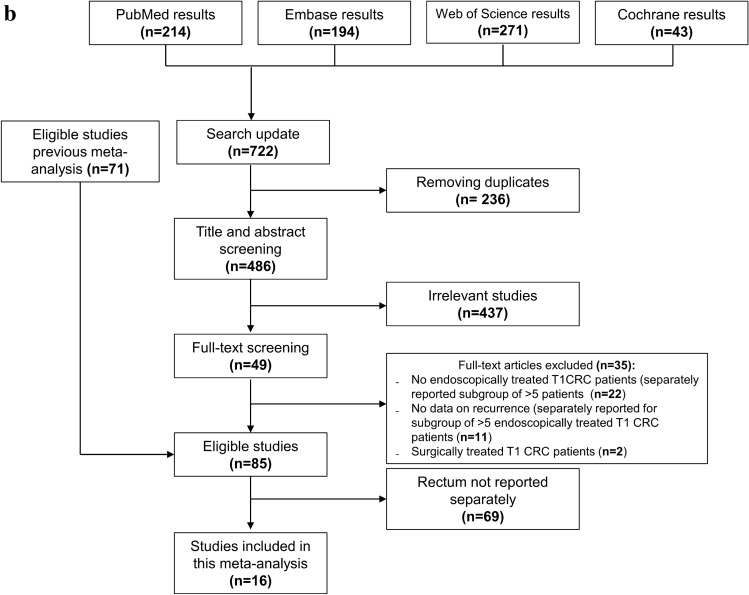
Methods: A systematic search was conducted for T1RC patients treated with local surgical resection. The primary outcome was the risk of RC recurrence and RC-related mortality. Pooled estimates were calculated using mixed-effect logistic regression. We also systematically searched and evaluated endoscopically treated T1RC patients in a similar manner.
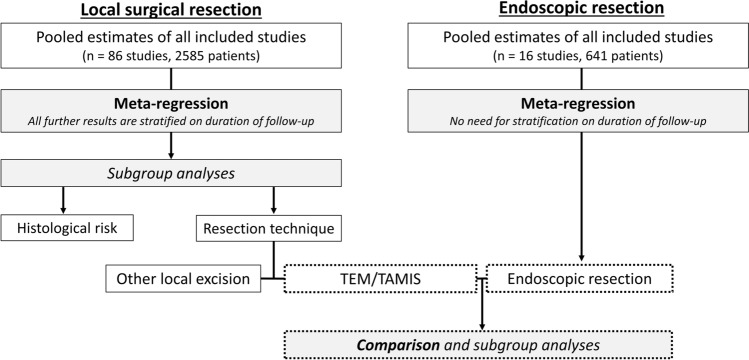
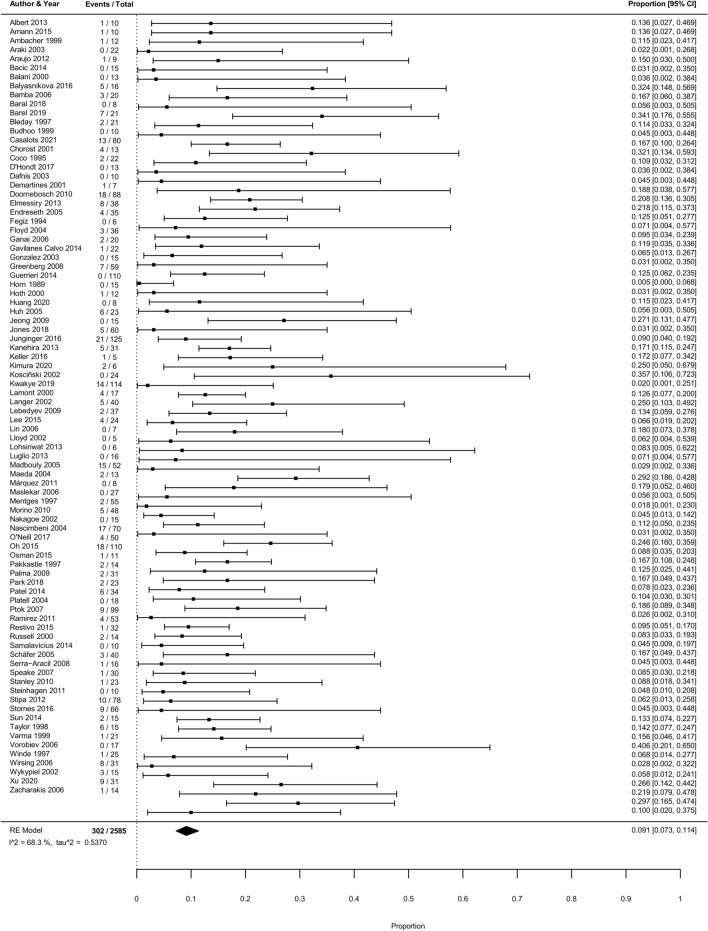
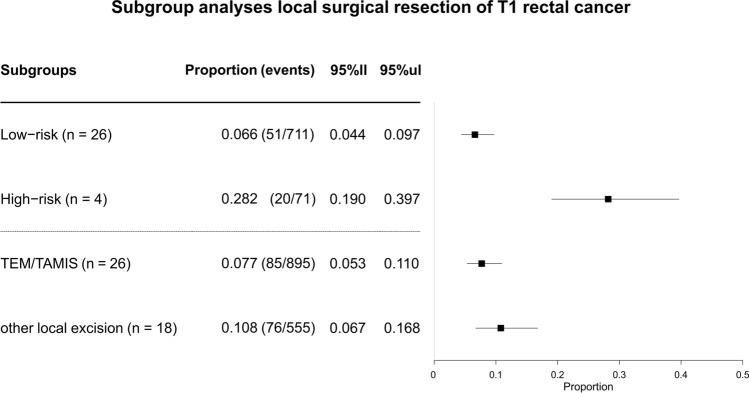
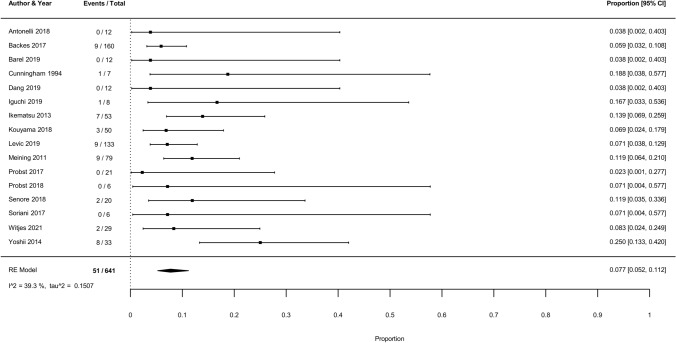
Results: In 2585 unique T1RC patients (86 studies) undergoing local surgical resection, the overall pooled cumulative incidence of recurrence was 9.1% (302 events, 95% CI 7.3-11.4%; I2 = 68.3%). In meta-regression, the recurrence risk was associated with histological risk status (p < 0.005; low-risk 6.6%, 95% CI 4.4-9.7% vs. high-risk 28.2%, 95% CI 19-39.7%) and local surgical resection technique (p < 0.005; TEM/TAMIS 7.7%, 95% CI 5.3-11.0% vs. other local surgical excisions 10.8%, 95% CI 6.7-16.8%). In 641 unique T1RC patients treated with flexible endoscopic excision (16 studies), the risk of recurrence (7.7%, 95% CI 5.2-11.2%), cancer-related mortality (2.3%, 95% CI 1.1-4.9), and cancer-related mortality among patients with recurrence (30.0%, 95% CI 14.7-49.4%) were comparable to outcomes after TEM/TAMIS (risk of recurrence 7.7%, 95% CI 5.3-11.0%, cancer-related mortality 2.8%, 95% CI 1.2-6.2% and among patients with recurrence 35.6%, 95% CI 21.9-51.2%).
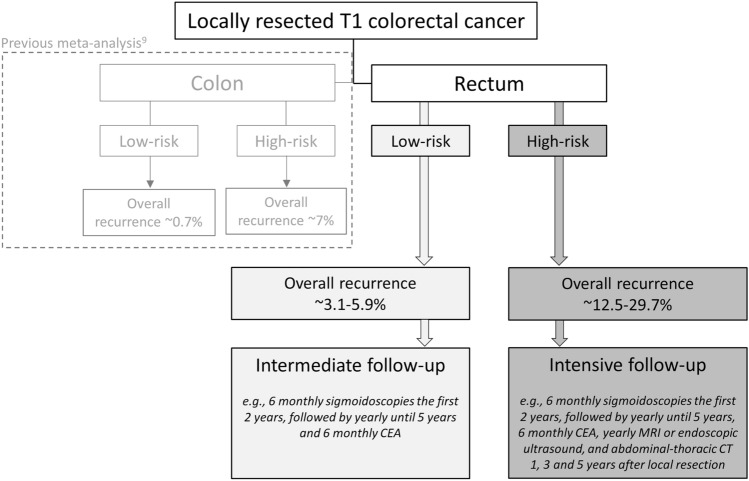
Conclusions: Patients with T1 rectal cancer may have a significantly lower recurrence risk after TEM/TAMIS compared to other local surgical resection techniques. After TEM/TAMIS and endoscopic resection the recurrence risk, cancer-related mortality and cancer-related mortality among patients with recurrence were comparable. Recurrence was mainly dependent on histological risk status.
Keywords: Follow-up; Local surgical resection; Recurrence; T1 rectal cancer; Therapeutic endoscopy.
© 2022. The Author(s).
Figures
References
-
- Dekker E, Tanis PJ, Vleugels JLA, et al. Colorectal cancer. Lancet. 2019;394(10207):1467–1480. - PubMed
-
- Lezoche E, Paganini AM, Fabiani B, et al. Quality-of-life impairment after endoluminal locoregional resection and laparoscopic total mesorectal excision. Surg Endosc. 2014;28(1):227–234. - PubMed
-
- Bennis M, Parc Y, Lefevre JH, et al. Morbidity risk factors after low anterior resection with total mesorectal excision and coloanal anastomosis: a retrospective series of 483 patients. Ann Surg. 2012;255(3):504–510. - PubMed
-
- van Groningen JT, van Hagen P, Tollenaar R, et al. Evaluation of a Completion Total Mesorectal Excision in Patients After Local Excision of Rectal Cancer: A Word of Caution. J Natl Compr Canc Netw. 2018;16(7):822–828. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
