

Re-interpreting mesenteric vascular anatomy on 3D virtual and/or physical models, part II: anatomy of relevance to surgeons operating splenic flexure cancer
- PMID: 35773607
- PMCID: PMC9652173
- DOI: 10.1007/s00464-022-09394-5
Re-interpreting mesenteric vascular anatomy on 3D virtual and/or physical models, part II: anatomy of relevance to surgeons operating splenic flexure cancer
Abstract
Background: The splenic flexure is irrigated from two vascular areas, both from the middle colic and the left colic artery. The challenge for the surgeon is to connect these two vascular areas in an oncological safe procedure.
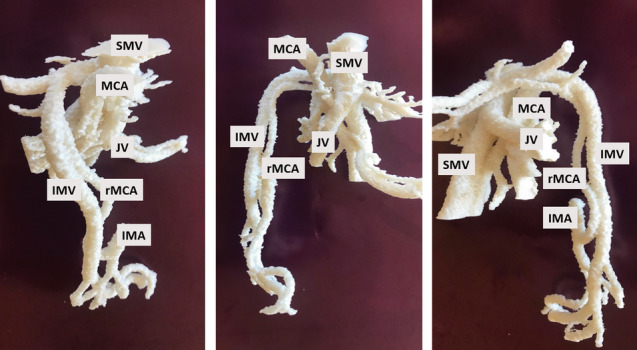
Materials and methods: The vascular anatomy, manually 3D reconstructed from 32 preoperative high-resolution CT datasets using Osirix MD, Mimics Medical and 3-matic Medical Datasets, were exported as STL-files, video clips, stills and supplemented with 3D printed models.
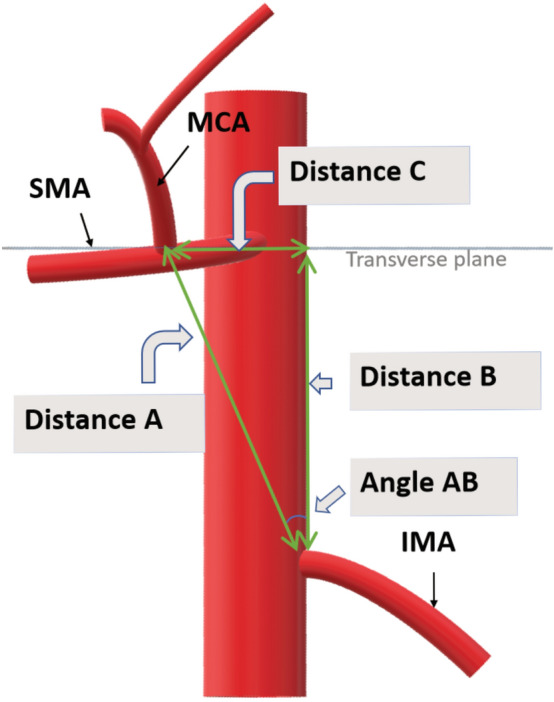
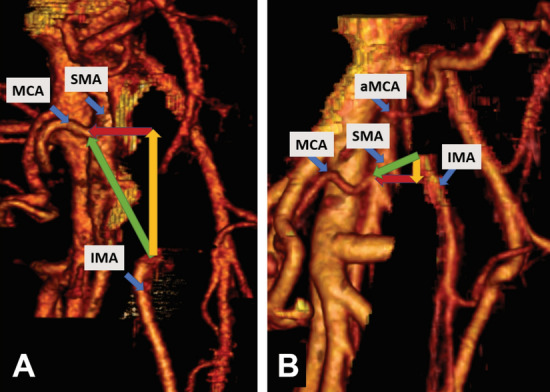
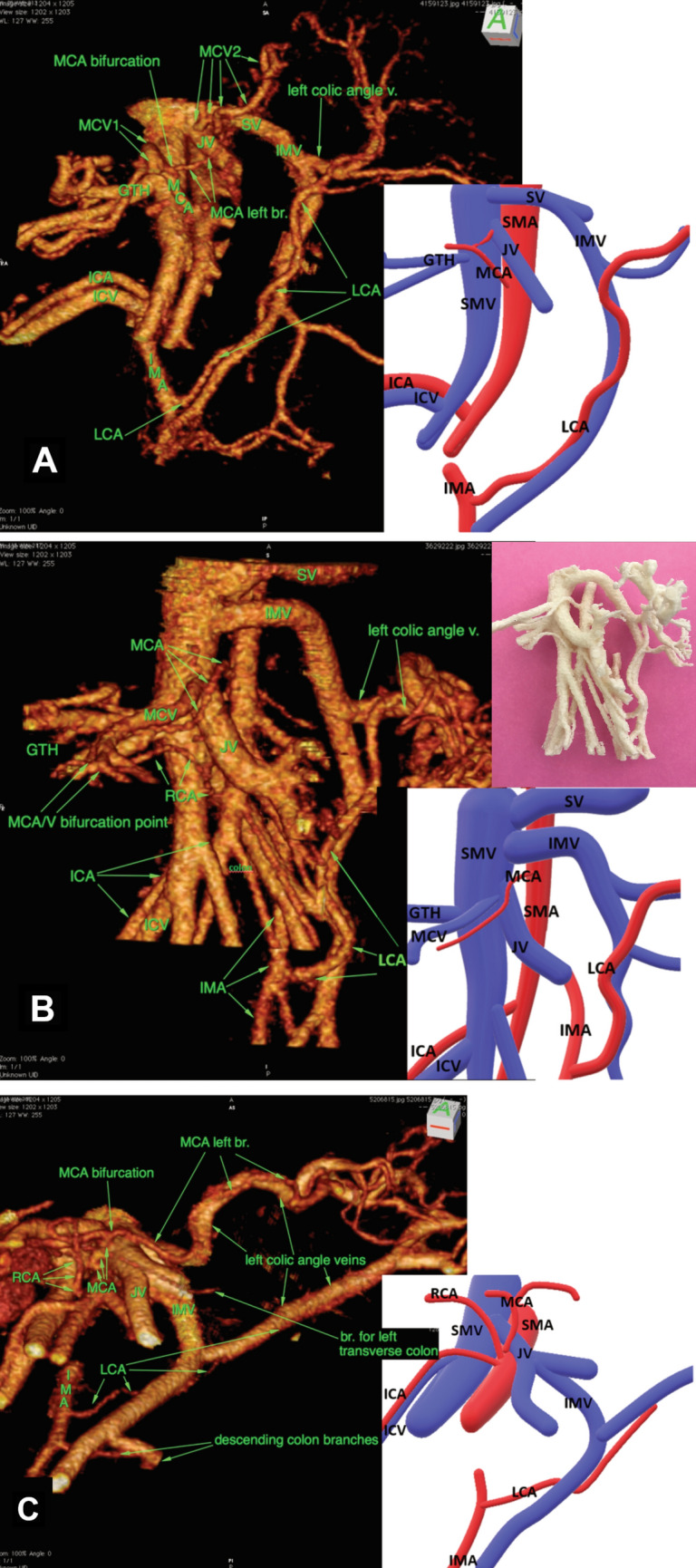
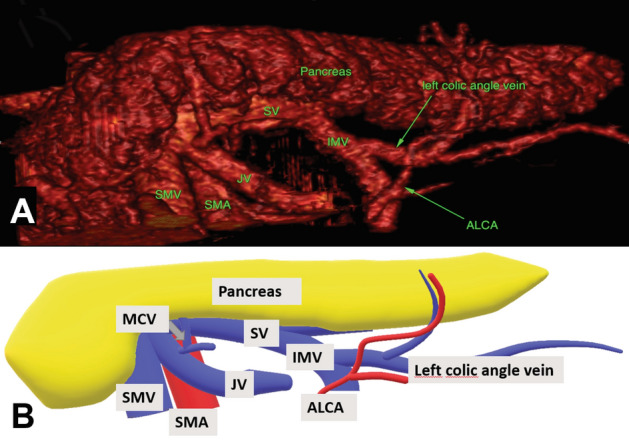
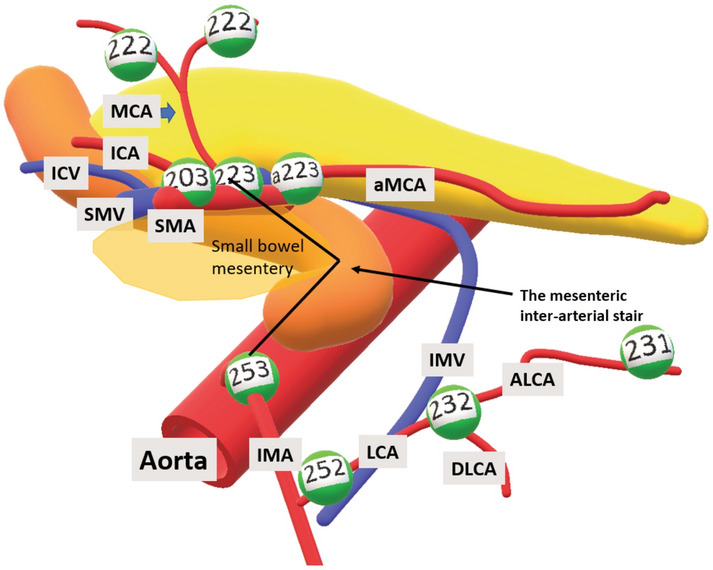
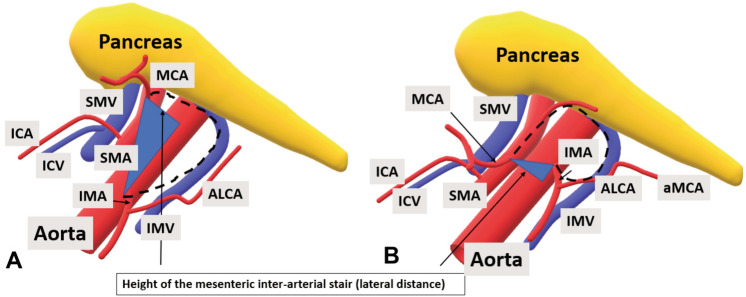
Results: Our first major finding was the difference in level between the middle colic and the inferior mesenteric artery origins. We have named this relationship a mesenteric inter-arterial stair. The middle colic artery origin could be found cranial (median 3.38 cm) or caudal (median 0.58 cm) to the inferior mesenteric artery. The lateral distance between the two origins was 2.63 cm (median), and the straight distance 4.23 cm (median). The second finding was the different trajectories and confluence pattern of the inferior mesenteric vein. This vein ended in the superior mesenteric/jejunal vein (21 patients) or in the splenic vein (11 patients). The inferior mesenteric vein confluence could be infrapancreatic (17 patients), infrapancreatic with retropancreatic arch (7 patients) or retropancreatic (8 patients). Lastly, the accessory middle colic artery was present in ten patients presenting another pathway for lymphatic dissemination.
Conclusion: The IMV trajectory when accessible, is the solution to the mesenteric inter-arterial stair. The surgeon could safely follow the IMV to its confluence. When the IMV trajectory is not accessible, the surgeon could follow the caudal border of the pancreas.
Keywords: D3 mesenterectomy; Inferior mesenteric artery; Left colectomy; Mesenteric vascular anatomy; Middle colic artery; Splenic flexure cancer.
© 2022. The Author(s).
Conflict of interest statement
Bjarte T. Andersen, Bojan V. Stimec, Airazat M. Kazaryan, Peter Rancinger, Bjørn Edwin, and Dejan Ignjatovic have no conflict of interest or financial ties to disclose.
Figures
References
-
- Sjo OH, Lunde OC, Nygaard K, Sandvik L, Nesbakken A. Tumour location is a prognostic factor for survival in colonic cancer patients. Colorectal Dis. 2008;10(1):33–40. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
