

Can diverse population characteristics be leveraged in a machine learning pipeline to predict resource intensive healthcare utilization among hospital service areas?
- PMID: 35773679
- PMCID: PMC9248096
- DOI: 10.1186/s12913-022-08154-4
Can diverse population characteristics be leveraged in a machine learning pipeline to predict resource intensive healthcare utilization among hospital service areas?
Abstract
Background: Super-utilizers represent approximately 5% of the population in the United States (U.S.) and yet they are responsible for over 50% of healthcare expenditures. Using characteristics of hospital service areas (HSAs) to predict utilization of resource intensive healthcare (RIHC) may offer a novel and actionable tool for identifying super-utilizer segments in the population. Consumer expenditures may offer additional value in predicting RIHC beyond typical population characteristics alone.
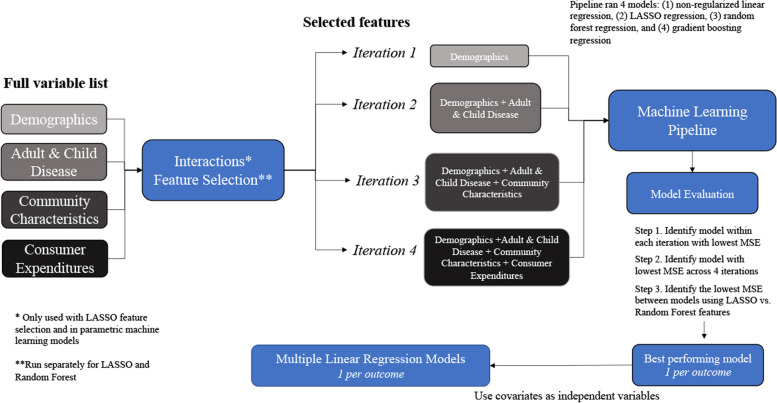
Methods: Cross-sectional data from 2017 was extracted from 5 unique sources. The outcome was RIHC and included emergency room (ER) visits, inpatient days, and hospital expenditures, all expressed as log per capita. Candidate predictors from 4 broad groups were used, including demographics, adults and child health characteristics, community characteristics, and consumer expenditures. Candidate predictors were expressed as per capita or per capita percent and were aggregated from zip-codes to HSAs using weighed means. Machine learning approaches (Random Forrest, LASSO) selected important features from nearly 1,000 available candidate predictors and used them to generate 4 distinct models, including non-regularized and LASSO regression, random forest, and gradient boosting. Candidate predictors from the best performing models, for each outcome, were used as independent variables in multiple linear regression models. Relative contribution of variables from each candidate predictor group to regression model fit were calculated.
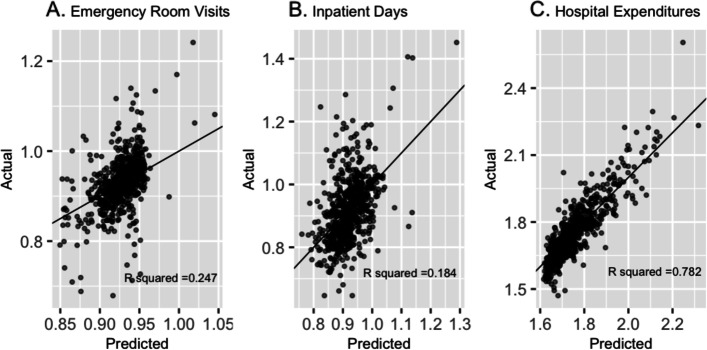
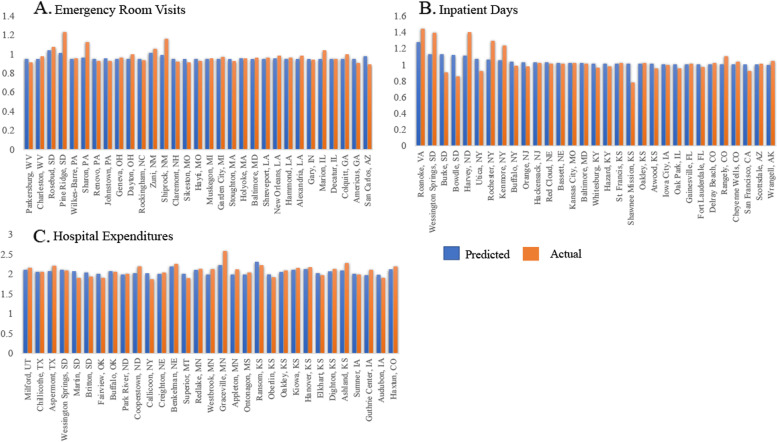
Results: The median ER visits per capita was 0.482 [IQR:0.351-0.646], the median inpatient days per capita was 0.395 [IQR:0.214-0.806], and the median hospital expenditures per capita was $2,302 [1$,544.70-$3,469.80]. Using 1,106 variables, the test-set coefficient of determination (R2) from the best performing models ranged between 0.184-0.782. The adjusted R2 values from multiple linear regression models ranged from 0.311-0.8293. Relative contribution of consumer expenditures to model fit ranged from 23.4-33.6%.
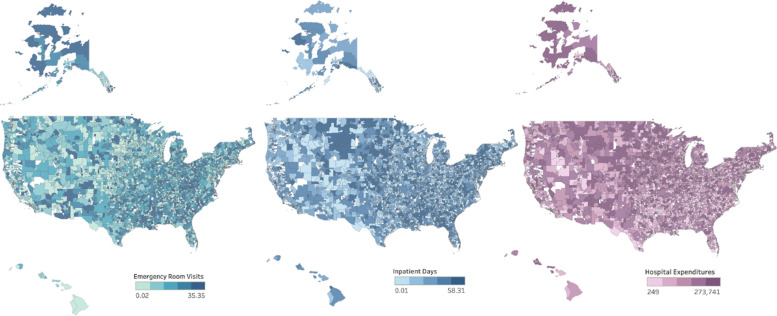
Discussion: Machine learning models predicted RIHC among HSAs using diverse population data, including novel consumer expenditures and provides an innovative tool to predict population-based healthcare utilization and expenditures. Geographic variation in utilization and spending were identified.
© 2022. The Author(s).
Conflict of interest statement
Ricket, IM: No potential conflicts exist. Ailawadi KL: No potential conflicts exist. Emond JA: No potential conflicts exist. MacKenzie TA: No potential conflicts exist. Brown JR: No potential conflicts exist.
Figures
References
-
- Centers for Medicare & Medicaid Services. Health Spending by Type of Service or Product. In: National Health Expenditures 2017 Highlights. Centers for Medicare & Medicaid Services. 2018. https://www.cms.gov/research-statistics-data-and-systems/statistics-tren.... Accessed 1 June 2020.
-
- Iovan S, Lantz PM, Allan K, Abir M. Interventions to Decrease Use in Prehospital and Emergency Care Settings Among Super-Utilizers in the United States: A Systematic Review. Med Care Res Rev. 2020;77(2):99-111.10.1177/1077558719845722. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
