

Performance of the 0-Hour/1-Hour Algorithm for Diagnosing Myocardial Infarction in Patients With Chest Pain in the Emergency Department - A Systematic Review and Meta-Analysis
- PMID: 35774074
- PMCID: PMC9168511
- DOI: 10.1253/circrep.CR-22-0001
Performance of the 0-Hour/1-Hour Algorithm for Diagnosing Myocardial Infarction in Patients With Chest Pain in the Emergency Department - A Systematic Review and Meta-Analysis
Abstract
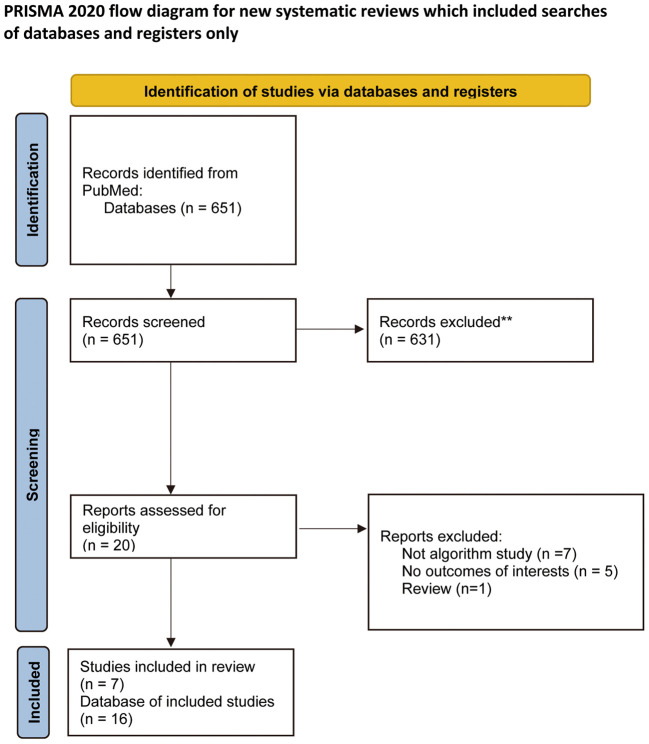
Background: This study assessed the diagnostic performance of the 0-hour/1-hour (0/1-h) algorithm to rule in and rule out acute myocardial infarction (MI) in patients presenting to the emergency department (ED) for suspected acute coronary syndrome without ST-segment elevation, as recommended in the 2015 European Society of Cardiology (ESC) guideline. Methods and Results: Following the Preferred Reporting Items for a Systematic Review and Meta-analysis of Diagnostic Test Accuracy (PRISMA-DTA) guidelines, a systematic review was conducted using the PubMed database from inception to March 31, 2020. We included any article published in English investigating the diagnostic performance of the ESC 0/1-h algorithm for diagnosing MI in patients with chest pain visiting the ED. Of 651 studies identified as potentially available for the study, 7 studies including 16 databases were analyzed. A meta-analysis of the diagnostic accuracy of the 0/1-h algorithm using high-sensitivity cardiac troponin I (hs-cTn) with 6 observational databases showed a pooled sensitivity of 99.3% (95% confidence interval [CI] 98.5-99.7%) and a pooled specificity of 90.1% (95% CI 80.7-95.2%). A meta-analysis of the diagnostic accuracy of 10 observational databases of the ESC 0/1-h algorithm using hs-cTn revealed a pooled sensitivity of 99.3% (95% CI 96.9-99.9%) and a pooled specificity of 91.7% (95% CI 83.5-96.1%). Conclusions: Our results demonstrate that the ESC 0/1-h algorithm can effectively rule in and rule out patients with non-ST-segment elevation MI.
Keywords: 0/1-h algorithm; High-sensitivity troponin; Pooled sensitivity; Pooled specificity; Suspected NSTEMI.
Copyright © 2022, THE JAPANESE CIRCULATION SOCIETY.
Conflict of interest statement
T. Matoba is a member of Circulation Reports’ Editorial Team. The other authors declare no conflicts of interest with regard to this article.
Figures


References
-
- Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, et al.. Fourth universal definition of myocardial infarction. Eur Heart J 2019; 40: 237–269. - PubMed
-
- Anderson JL, Adams CD, Antman EM, Bridges CR, Califf RM, Casey DE Jr, et al.. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-elevation myocardial infarction: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients with Unstable Angina/Non-ST-elevation Myocardial Infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. J Am Coll Cardiol 2007; 50: e1–e157. - PubMed
-
- Alpert JS, Thygesen K, Antman E, Bassand JP.. Myocardial infarction redefined: A consensus document of the Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. Eur Heart J 2000; 21: 1502–1513. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials