

A Systematic Review of Ovarian Tissue Transplantation Outcomes by Ovarian Tissue Processing Size for Cryopreservation
- PMID: 35774145
- PMCID: PMC9239173
- DOI: 10.3389/fendo.2022.918899
A Systematic Review of Ovarian Tissue Transplantation Outcomes by Ovarian Tissue Processing Size for Cryopreservation
Abstract
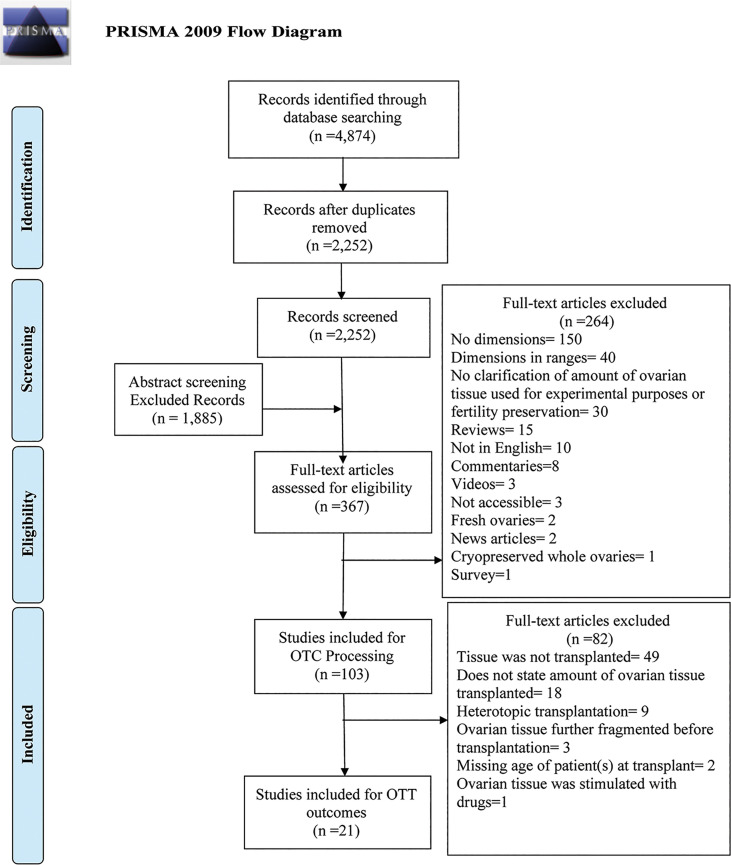
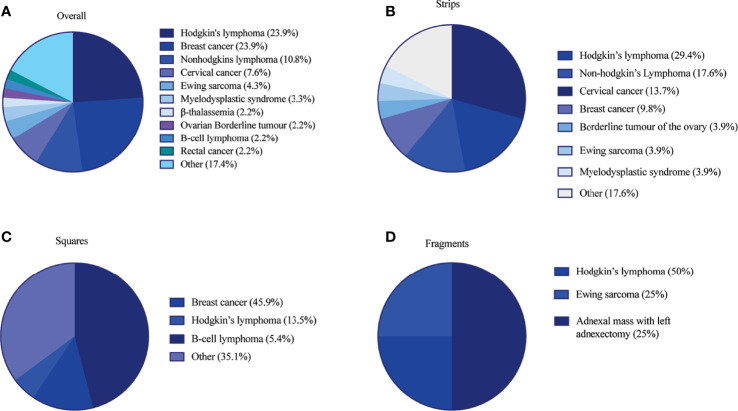
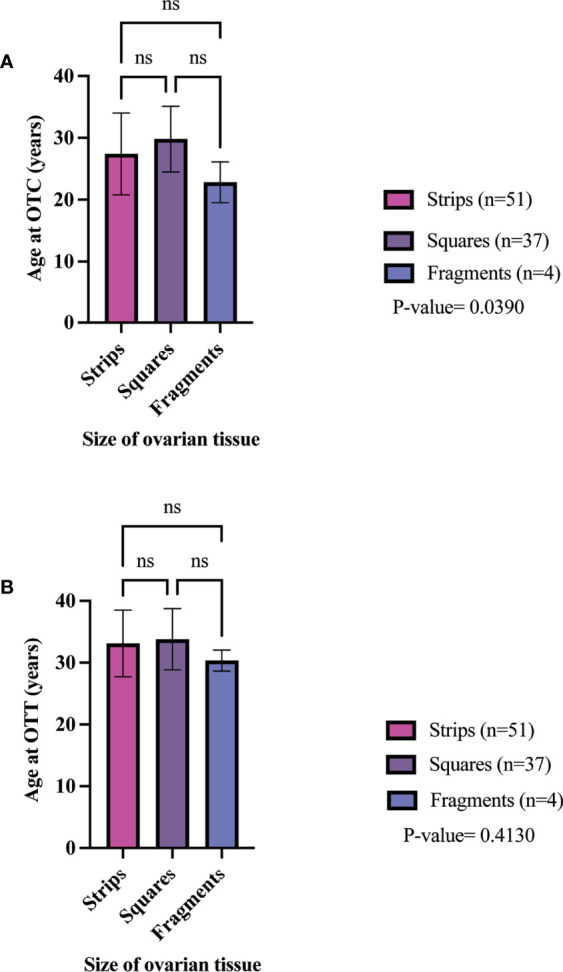
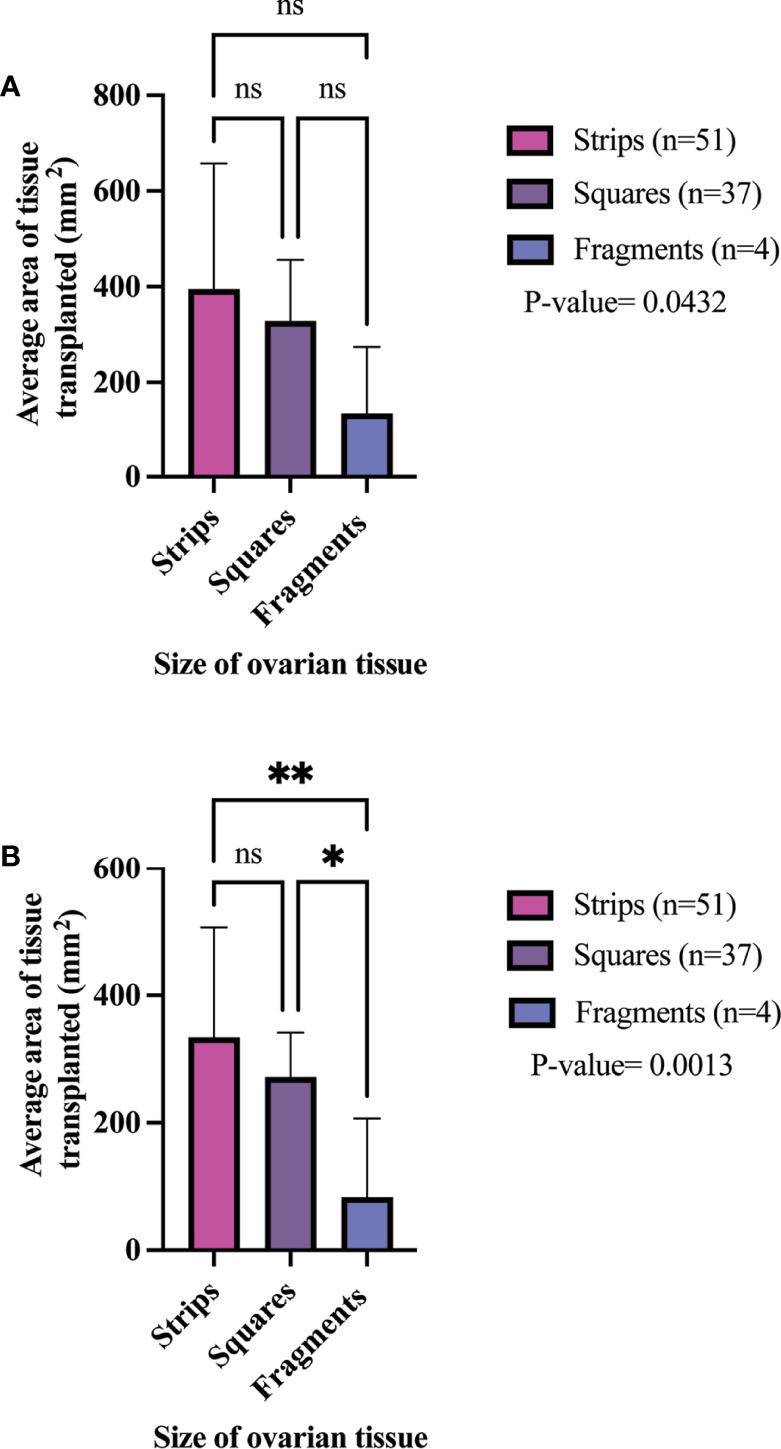
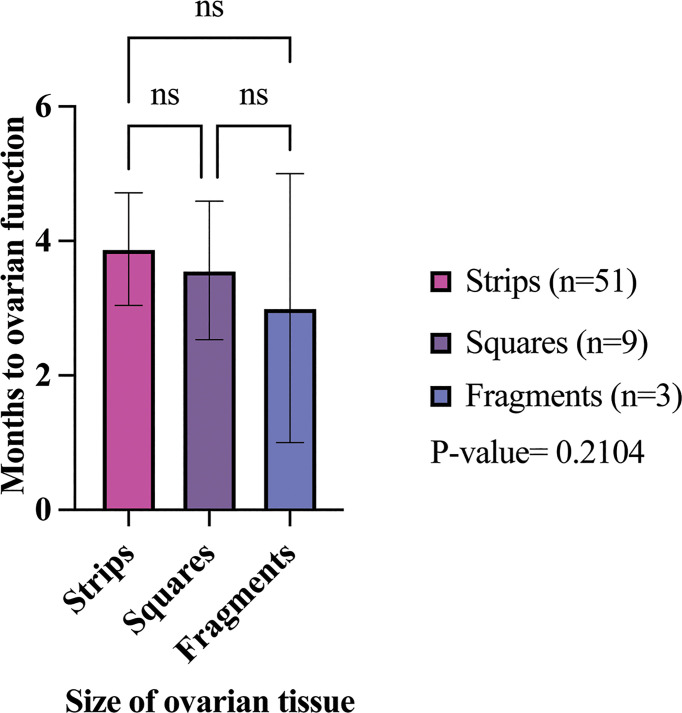
Ovarian tissue cryopreservation (OTC) is the only pre-treatment option currently available to preserve fertility for prepubescent girls and patients who cannot undergo ovarian stimulation. Currently, there is no standardized method of processing ovarian tissue for cryopreservation, despite evidence that fragmentation of ovaries may trigger primordial follicle activation. Because fragmentation may influence ovarian transplant function, the purpose of this systematic review was (1) to identify the processing sizes and dimensions of ovarian tissue within sites around the world, and (2) to examine the reported outcomes of ovarian tissue transplantation including, reported duration of hormone restoration, pregnancy, and live birth. A total of 2,252 abstracts were screened against the inclusion criteria. In this systematic review, 103 studies were included for analysis of tissue processing size and 21 studies were included for analysis of ovarian transplantation outcomes. Only studies where ovarian tissue was cryopreserved (via slow freezing or vitrification) and transplanted orthotopically were included in the review. The size of cryopreserved ovarian tissue was categorized based on dimensions into strips, squares, and fragments. Of the 103 studies, 58 fertility preservation sites were identified that processed ovarian tissue into strips (62%), squares (25.8%), or fragments (31%). Ovarian tissue transplantation was performed in 92 participants that had ovarian tissue cryopreserved into strips (n = 51), squares (n = 37), and fragments (n = 4). All participants had ovarian tissue cryopreserved by slow freezing. The pregnancy rate was 81.3%, 45.5%, 66.7% in the strips, squares, fragment groups, respectively. The live birth rate was 56.3%, 18.2%, 66.7% in the strips, squares, fragment groups, respectively. The mean time from ovarian tissue transplantation to ovarian hormone restoration was 3.88 months, 3.56 months, and 3 months in the strips, squares, and fragments groups, respectively. There was no significant difference between the time of ovarian function' restoration and the size of ovarian tissue. Transplantation of ovarian tissue, regardless of its processing dimensions, restores ovarian hormone activity in the participants that were reported in the literature. More detailed information about the tissue processing size and outcomes post-transplant are required to identify a preferred or more successful processing method.
Systematic review registration: [https://www.crd.york.ac.uk], identifier [CRD42020189120].
Keywords: fertility preservation; oncofertility; ovarian tissue cryopreservation; ovarian tissue size; ovarian tissue transplantation.
Copyright © 2022 Diaz, Kubo, Handa, Hanna and Laronda.
Conflict of interest statement
ML is an Advisor for Dimension Inx, LLC. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Successful fertility preservation following ovarian tissue vitrification in patients with primary ovarian insufficiency.Hum Reprod. 2015 Mar;30(3):608-15. doi: 10.1093/humrep/deu353. Epub 2015 Jan 6. Hum Reprod. 2015. PMID: 25567618
-
Fresh and cryopreserved ovarian tissue transplantation for preserving reproductive and endocrine function: a systematic review and individual patient data meta-analysis.Hum Reprod Update. 2022 May 2;28(3):400-416. doi: 10.1093/humupd/dmac003. Hum Reprod Update. 2022. PMID: 35199164 Free PMC article.
-
Safeguarding Fertility With Whole Ovary Cryopreservation and Microvascular Transplantation: Higher Follicular Survival With Vitrification Than With Slow Freezing in a Ewe Model.Transplantation. 2016 Sep;100(9):1889-97. doi: 10.1097/TP.0000000000001296. Transplantation. 2016. PMID: 27336395
-
Ninety-five orthotopic transplantations in 74 women of ovarian tissue after cytotoxic treatment in a fertility preservation network: tissue activity, pregnancy and delivery rates.Hum Reprod. 2016 Sep;31(9):2031-41. doi: 10.1093/humrep/dew165. Epub 2016 Jul 4. Hum Reprod. 2016. PMID: 27378768
-
Autotransplantation of cryopreserved ovarian tissue--effective method of fertility preservation in cancer patients.Gynecol Endocrinol. 2014 Oct;30 Suppl 1:43-7. doi: 10.3109/09513590.2014.945789. Gynecol Endocrinol. 2014. PMID: 25200829 Review.
Cited by
-
Ovarian tissue transplantation: 10 years of experience at the Bologna University.Front Endocrinol (Lausanne). 2024 Mar 7;15:1332673. doi: 10.3389/fendo.2024.1332673. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 38516411 Free PMC article.
-
Prevention and management of radiotherapy-related toxicities in gynecological malignancies. Position paper on behalf of AIRO (Italian Association of Radiotherapy and Clinical Oncology).Radiol Med. 2024 Sep;129(9):1329-1351. doi: 10.1007/s11547-024-01844-5. Epub 2024 Aug 28. Radiol Med. 2024. PMID: 39198369 Free PMC article.
-
Research progress on mechanism of follicle injury after ovarian tissue transplantation and protective strategies.Zhejiang Da Xue Xue Bao Yi Xue Ban. 2024 Apr 1;53(3):321-330. doi: 10.3724/zdxbyxb-2023-0566. Zhejiang Da Xue Xue Bao Yi Xue Ban. 2024. PMID: 38562041 Free PMC article. Review. Chinese, English.
-
Reproductive and Obstetric Outcomes after Fertility-Sparing Treatments for Cervical Cancer: Current Approach and Future Directions.J Clin Med. 2023 Mar 30;12(7):2614. doi: 10.3390/jcm12072614. J Clin Med. 2023. PMID: 37048696 Free PMC article. Review.
-
Generation of Tailored Extracellular Matrix Hydrogels for the Study of In Vitro Folliculogenesis in Response to Matrisome-Dependent Biochemical Cues.Bioengineering (Basel). 2024 May 25;11(6):543. doi: 10.3390/bioengineering11060543. Bioengineering (Basel). 2024. PMID: 38927779 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources