

Impact of a Six-Week Prehabilitation With Blood-Flow Restriction Training on Pre- and Postoperative Skeletal Muscle Mass and Strength in Patients Receiving Primary Total Knee Arthroplasty
- PMID: 35774280
- PMCID: PMC9237436
- DOI: 10.3389/fphys.2022.881484
Impact of a Six-Week Prehabilitation With Blood-Flow Restriction Training on Pre- and Postoperative Skeletal Muscle Mass and Strength in Patients Receiving Primary Total Knee Arthroplasty
Abstract
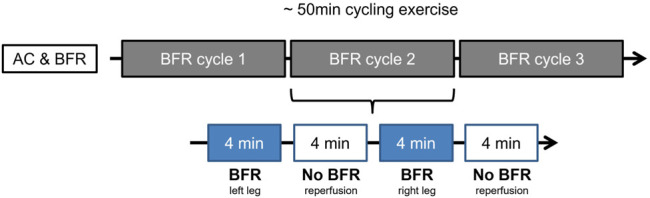
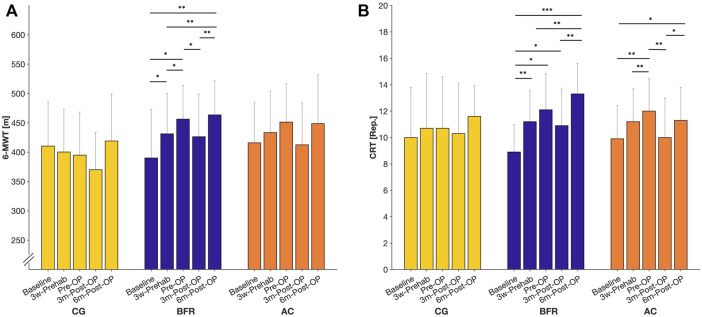
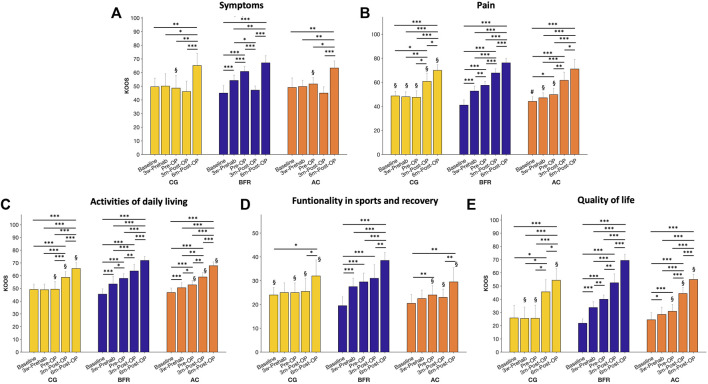
Introduction: Total Knee Arthroplasty (TKA) is one of the most successful interventions in gonarthrosis, however the operation is leading to muscle atrophy and long-term muscular deficits. To enhance rehabilitation after TKA, exercise programs try to improve muscle function preoperatively, called prehabilitation. Blood-Flow-Restriction Exercises (BFRE) is a training method which is characterized by using tourniquets to reduce arterial and occlude venous blood flow simultaneously during the exercise to increase metabolic stress. The present study aimed to evaluate the effects of a 6-week prehabilitation with BFR on pre- and postoperative muscle mass, strength, and quality of life (QoL). Methods: 30 patients with end-stage gonarthrosis participated in this study. Patients were randomized into one of three groups: 1) Control-Group (CON): Standard clinical approach without prehabilitation. 2) Active-Control-Group (AC): Participation in a prehabilitation with sham-BFR. 3) BFR-Group (BFR): Participation in a prehabilitation with BFR. The prehabilitation protocol consist of a cycling-ergometer-based training performed twice per week over 6 weeks. During exercise, BFR was applied periodically three times per leg with a pressure of 40% of the individual-limb-occlusion-pressure. Measurement time points were six- (baseline), 3-weeks and 5-days before the surgery (Pre-OP), as well as three- and 6-months postoperatively. Outcome measures were muscular strength of the thigh muscles, thigh circumference as well as QoL and functional activity, examined by 6-min walking- and chair rising test. Results: Both training groups indicated significantly improved leg muscle strength following the prehabilitation period with a superior effect for the BFR-group (BFR: ∼170% vs. AC: ∼91%, p < 0.05). No significant changes in leg strength occurred in the CON (∼3%, p = 0.100). Further, patients in BFR-group indicated significantly improved skeletal muscle mass assessed by femoral circumference following prehabilitation period (∼7%, p < 0.05), while no significant changes occurred in the CON (-1.14%, p = 0.131) and AC-group (∼3%, p = 0.078). At 3-months Post-OP, the CON and BFR-group revealed a significant decrease in femoral circumference compared to the Pre-OP (CON: ∼3%, BFR: ∼4%; p < 0.05), but BFR-group remained above the baseline level (∼3%, p < 0.05). No significant change in femoral circumference was found for AC-group (∼2%, p = 0.078). In addition, the prehabilitation with BFR provided notably improved Knee Injury and Osteoarthritis Outcome Scores (KOOS) especially in pain perception with significant higher effect compared to other groups (CON: -2%, AC: 13%, BFR: 41%; p < 0.05). In long-term rehabilitation after 6-months, all groups showed significantly improved KOOS scores in all dimensions (CON: ∼110%, AC: ∼132%, BFR: ∼225%; p < 0.01), and functional examinations (CON: ∼26%, AC: ∼16%, BFR: ∼53%; p < 0.01). Conclusion: The present findings show that BFR-prehabilitation induce significant improvements in muscle function and QoL before TKA surgery. In addition, the supporting effect of prehabilitation on postoperative regeneration and QoL should be highlighted, illustrating prolonged beneficial effects of BFR on muscular and functional performance in a "better in, better out"-manner.
Keywords: exercise therapy; kaatsu training; muscle atrophy; rehabilitation; venous occlusion.
Copyright © 2022 Franz, Ji, Bittersohl, Zilkens and Behringer.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Calatayud J., Casaña J., Ezzatvar Y., Jakobsen M. D., Sundstrup E., Andersen L. L. (2017). High-intensity Preoperative Training Improves Physical and Functional Recovery in the Early Post-operative Periods after Total Knee Arthroplasty: a Randomized Controlled Trial. Knee Surg. Sports Traumatol. Arthrosc. 25, 2864–2872. 10.1007/s00167-016-3985-5 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous