

Effect of Adding Vertical Correction to Dynamic Scapular Recognition on Scapular Dyskinesis and Shoulder Disability in Patients With Adhesive Capsulitis: A Randomized Clinical Study
- PMID: 35774629
- PMCID: PMC9237598
- DOI: 10.1016/j.jcm.2022.02.002
Effect of Adding Vertical Correction to Dynamic Scapular Recognition on Scapular Dyskinesis and Shoulder Disability in Patients With Adhesive Capsulitis: A Randomized Clinical Study
Abstract
Objective: The purpose of this study was to measure the effect of adding vertical downward correction to dynamic scapular recognition exercise on scapular dyskinesis and shoulder pain and disability in people with adhesive capsulitis.
Methods: Sixty-seven participants with adhesive capsulitis were randomized into 2 groups. The taping intervention group performed a dynamic scapular recognition exercise using a wireless biofeedback system and a continual vertical downward correction using rigid taping with 50% to 75% tension. The comparison group performed a similar dynamic scapular recognition exercise but with sham taping. The primary outcome measures were scapular dyskinesis, scapular upward rotation, and Shoulder Pain and Disability Index, and the secondary outcome measures were shoulder flexion, abduction, and external rotation.
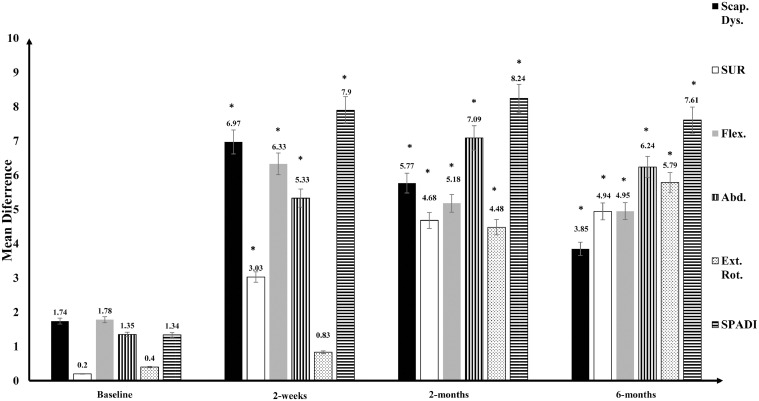
Results: After 2 weeks, there were significant differences between the taping intervention group and the comparison group in scapular dyskinesis, scapular upward rotation, shoulder flexion, abduction, and Shoulder Pain and Disability Index (P < .05), and nonsignificant differences in shoulder external rotation (P > .05). After 2 and 6 months, there were significant differences between groups in all dependent outcome measures (P < .05).
Conclusion: This study demonstrated that from adding taping with a vertical downward correction to dynamic scapular recognition exercises, significant short-term and long-term improvements in scapular dyskinesis and shoulder pain and disability in people with adhesive capsulitis were observed. These improvements persisted for 6 months after intervention.
Keywords: Bursitis; Dyskinesias; Rehabilitation; Shoulder.
© 2022 by National University of Health Sciences.
Figures





References
-
- Neviaser AS, Hannafin JA. Adhesive capsulitis: a review of current treatment. Am J Sports Med. 2010;38(11):2346–2356. - PubMed
LinkOut - more resources
Full Text Sources
Medical
