

Right-sided aortic arch with Kommerell's diverticulum: a case report of a rare cause of type B dissection
- PMID: 35775016
- PMCID: PMC9237716
- DOI: 10.1093/ehjcr/ytac238
Right-sided aortic arch with Kommerell's diverticulum: a case report of a rare cause of type B dissection
Abstract
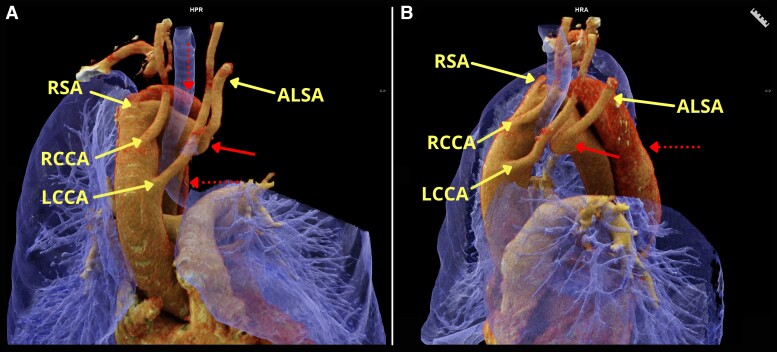
Background: A right-sided aortic arch (RAArch) is present in approximately 0.1% of the population. A Kommerell's diverticulum (KD), a remnant of the dorsal aortic arch usually refers to an aneurysmal aortic enlargement at the origin of an aberrant left subclavian artery (ALSA) and is associated with an increased risk of aortic dissection.
Case summary: A 59-year-old female smoker with a history of hypertension and hypercholesterolaemia presented with a 24-hour history of sudden-onset and severe stabbing chest pain radiating to the interscapular region. Physical examination was normal except for bilateral basal crepitations. Computed tomography angiography (CTA) showed a type B aortic dissection in a RAArch with an ALSA arising from KD with a peri-aortic haematoma and haemothorax without any active contrast extravasation. After medical stabilization, a semi-urgent hybrid repair was performed with a right carotid-subclavian bypass, thoracic endovascular aortic repair (TEVAR), a plug in the left subclavian artery, and left carotid-subclavian bypass due to severe ischaemia of the left arm. The postoperative CTA showed patent bypasses, aortic remodelling, and a minimal type IIa endoleak at the level of the ALSA.
Discussion: In patients with a type B dissection and KD, hybrid repair including TEVAR is feasible after careful pre-operative assessment of the patient's unique anatomy and may reduce post-surgical morbidity and mortality compared to open surgery. Prophylactic repair may be considered in patients with an asymptomatic RAArch and KD.
Keywords: Acute aortic syndrome; Aortic dissection; Case report; Congenital aortic anomaly; Kommerell's diverticulum; Right-sided aortic arch.
© The Author(s) 2022. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures




References
-
- Edwards JE. Anomalies of the derivatives of the aortic arch system. Med Clin North Am 1948;32:925–949. - PubMed
-
- Tanaka A, Milner R, Ota T. Kommerell's diverticulum in the current era: a comprehensive review. Gen Thorac Cardiovasc Surg 2015;63:245–259. - PubMed
-
- Stewart JR, Kincaid OW, Titus JL. Right aortic arch: plain film diagnosis and significance. Am J Roentgenol Radium Ther Nucl Med 1966;97:377–389. - PubMed
-
- Tyczyński P, Michałowska I, Wolny R, Dobrowolski P, Łazarczyk H, Rybicka J, Hoffman P, Witkowski A. Left aberrant subclavian artery. Systematic study in adult patients. Int J Cardiol 2017;240:183–186. - PubMed
Publication types
LinkOut - more resources
Full Text Sources