

Care Disruptions and End-Of-Life Care Experiences Among Home-Based Primary Care Patients During the COVID-19 Pandemic in New York City: A Retrospective Chart Review
- PMID: 35775300
- PMCID: PMC9253522
- DOI: 10.1177/10499091221104732
Care Disruptions and End-Of-Life Care Experiences Among Home-Based Primary Care Patients During the COVID-19 Pandemic in New York City: A Retrospective Chart Review
Abstract
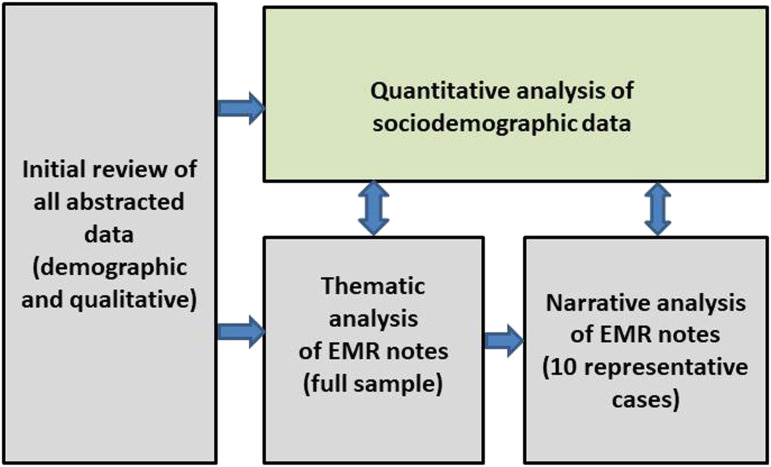
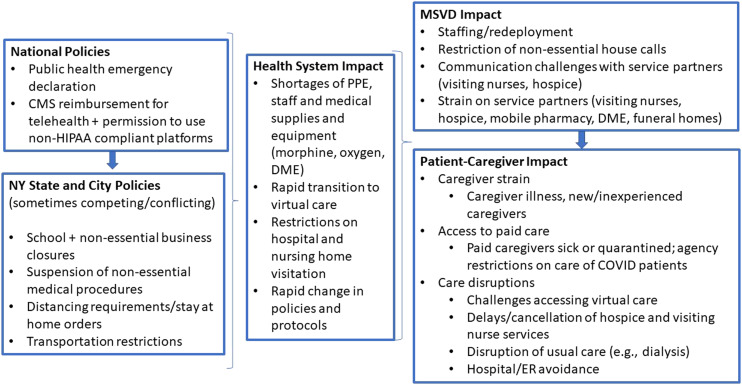
Background: Research on deaths during COVID-19 has largely focused on hospitals and nursing homes. Less is known about medically complex patients receiving care in the community. We examined care disruptions and end-of-life experiences of homebound patients receiving home-based primary care (HBPC) in New York City during the initial 2020 COVID-19 surge. Methods: We conducted a retrospective chart review of patients enrolled in Mount Sinai Visiting Doctors who died between March 1-June 30, 2020. We collected patient sociodemographic and clinical data and analyzed care disruptions and end-of-life experiences using clinical notes, informed by thematic and narrative analysis. Results: Among 1300 homebound patients, 112 (9%) died during the study period. Patients who died were more likely to be older, non-Hispanic white, and have dementia than those who survived. Thirty percent of decedents had confirmed or probable COVID-19. Fifty-eight (52%) were referred to hospice and 50 enrolled. Seventy-three percent died at home. We identified multiple intersecting disruptions in family caregiving, paid caregiving, medical supplies and services, and hospice care, as well as hospital avoidance, complicating EOL experiences. The HBPC team responded by providing clinical, logistical and emotional support to patients and families. Conclusion: Despite substantial care disruptions, the majority of patients in our study died at home with support from their HBPC team as the practice worked to manage care disruptions. Our findings suggest HBPC's multi-disciplinary, team-based model may be uniquely suited to meet the needs of the most medically and socially vulnerable older adults at end of life during public health emergencies.
Keywords: COVID-19; community-based care; end-of-life; home-based medical care; home-based primary care; homebound.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. This article does not reflect the views of the US Department of Veterans Affairs or the US government.
Figures
Similar articles
-
Disruptions in Home Hospice Care due to the COVID-19 Pandemic.J Palliat Med. 2023 Feb;26(2):244-247. doi: 10.1089/jpm.2022.0037. Epub 2022 Nov 17. J Palliat Med. 2023. PMID: 36394438 Free PMC article.
-
"At Home, with Care": Lessons from New York City Home-based Primary Care Practices Managing COVID-19.J Am Geriatr Soc. 2021 Feb;69(2):300-306. doi: 10.1111/jgs.16952. Epub 2020 Nov 20. J Am Geriatr Soc. 2021. PMID: 33179761 Free PMC article.
-
Disruptions in Care and Support for Homebound Adults in Home-Based Primary Care in New York City During the COVID-19 Pandemic.Home Healthc Now. 2021 Jul-Aug 01;39(4):211-214. doi: 10.1097/NHH.0000000000000983. Home Healthc Now. 2021. PMID: 34190705 Free PMC article.
-
A clinical microsystem model to evaluate the quality of primary care for homebound older adults.J Am Med Dir Assoc. 2009 Jun;10(5):304-13. doi: 10.1016/j.jamda.2009.02.003. J Am Med Dir Assoc. 2009. PMID: 19497542 Review.
-
A multidisciplinary program for delivering primary care to the underserved urban homebound: looking back, moving forward.J Am Geriatr Soc. 2006 Aug;54(8):1283-9. doi: 10.1111/j.1532-5415.2006.00835.x. J Am Geriatr Soc. 2006. PMID: 16914000 Review.
Cited by
-
Navigating a "Good Death" During COVID-19: Understanding Real-Time End-of-Life Care Structures, Processes, and Outcomes Through Clinical Notes.Gerontologist. 2024 Oct 1;64(10):gnae099. doi: 10.1093/geront/gnae099. Gerontologist. 2024. PMID: 39187989
-
Challenges in Care for Non-COVID-19 Patients with Severe Chronic Illnesses during COVID-19 Pandemic: A Qualitative Study of Healthcare Providers Working around Acute Care Hospitals in South Korea.Healthcare (Basel). 2023 Feb 17;11(4):611. doi: 10.3390/healthcare11040611. Healthcare (Basel). 2023. PMID: 36833145 Free PMC article.
-
Care disruptions among the homebound during the COVID-19 pandemic: An analysis of the role of dementia.J Am Geriatr Soc. 2022 Dec;70(12):3585-3592. doi: 10.1111/jgs.18008. Epub 2022 Aug 23. J Am Geriatr Soc. 2022. PMID: 35997146 Free PMC article.
-
Need of community-based palliative care in rural India and factors that influence its sustainability: a comprehensive exploration using qualitative methodology in rural Puducherry, India.Palliat Care Soc Pract. 2023 Sep 6;17:26323524231196315. doi: 10.1177/26323524231196315. eCollection 2023. Palliat Care Soc Pract. 2023. PMID: 37692560 Free PMC article.
-
Characteristics Associated With Homebound Vaccination Against COVID-19.J Am Med Dir Assoc. 2024 Sep;25(9):105147. doi: 10.1016/j.jamda.2024.105147. Epub 2024 Jul 11. J Am Med Dir Assoc. 2024. PMID: 39004101 Free PMC article.
References
-
- Reckrey JM, Yang M, Kinosian B, Bollens-Lund E, Leff B, Ritchie C, et al.Receipt of home-based medical care among older beneficiaries enrolled in fee-for-service Medicare: Study examines receipt of home-based medical care among community-dwelling, fee-for-service medicare beneficiaries age sixty-five or older. Health Aff. 2020;39(8):1289-1296. - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
