A point-prevalence study on community and inpatient Clostridioides difficile infections (CDI): results from Combatting Bacterial Resistance in Europe CDI (COMBACTE-CDI), July to November 2018
- PMID: 35775426
- PMCID: PMC9248264
- DOI: 10.2807/1560-7917.ES.2022.27.26.2100704
A point-prevalence study on community and inpatient Clostridioides difficile infections (CDI): results from Combatting Bacterial Resistance in Europe CDI (COMBACTE-CDI), July to November 2018
Abstract
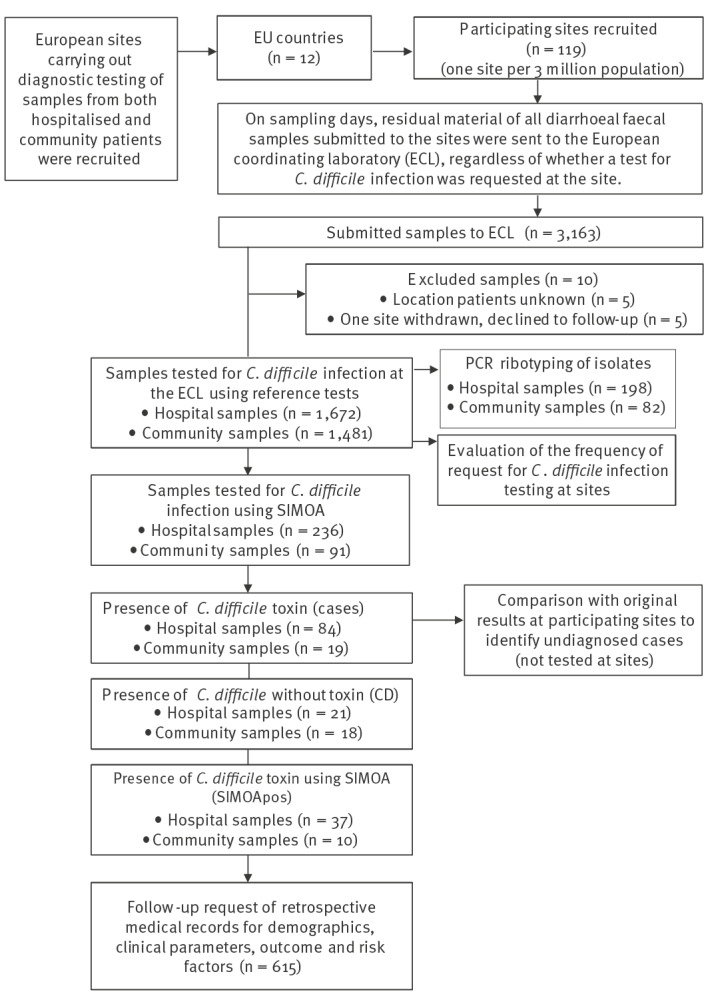
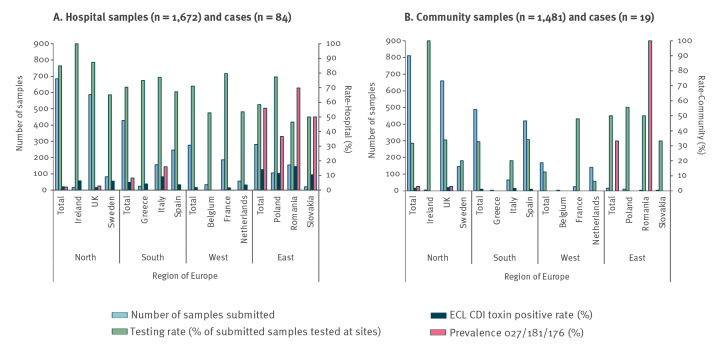
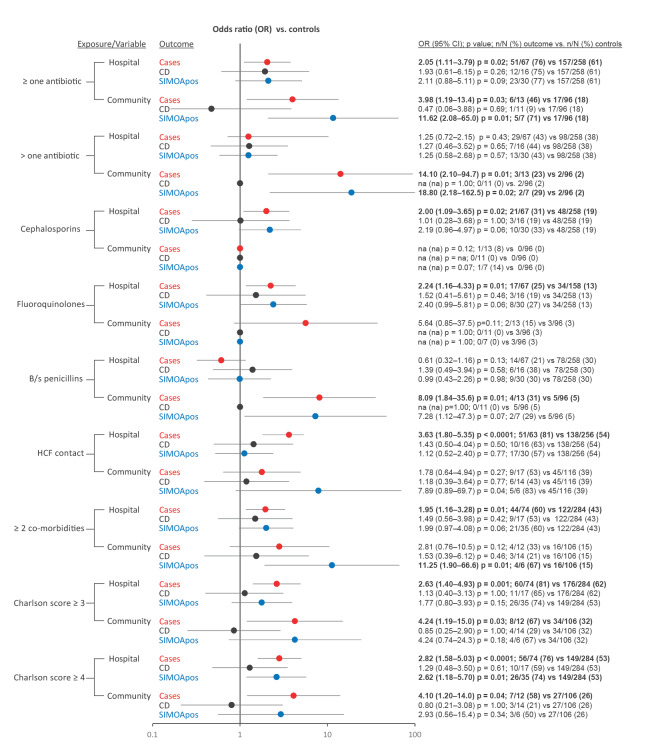
BackgroundThere is a paucity of data on community-based Clostridioides difficile infection (CDI) and how these compare with inpatient CDI.AimTo compare data on the populations with CDI in hospitals vs the community across 12 European countries.MethodsFor this point-prevalence study (July-November 2018), testing sites sent residual diagnostic material on sampling days to a coordinating laboratory for CDI testing and PCR ribotyping (n = 3,163). Information on whether CDI testing was requested at the original site was used to identify undiagnosed CDI. We used medical records to identify differences between healthcare settings in patient demographics and risk factors for detection of C. difficile with or without free toxin.ResultsThe CDI positivity rate was 4.4% (country range: 0-16.2) in hospital samples, and 1.3% (country range: 0-2.2%) in community samples. The highest prevalence of toxinotype IIIb (027, 181 and 176) was seen in eastern European countries (56%; 43/77), the region with the lowest testing rate (58%; 164/281). Different predisposing risk factors were observed (use of broad-spectrum penicillins in the community (OR: 8.09 (1.9-35.6), p = 0.01); fluoroquinolones/cephalosporins in hospitals (OR: 2.2 (1.2-4.3), p = 0.01; OR: 2.0 (1.1-3.7), p = 0.02)). Half of community CDI cases were undetected because of absence of clinical suspicion, accounting for three times more undiagnosed adults in the community compared with hospitals (ca 111,000 vs 37,000 cases/year in Europe).ConclusionThese findings support recommendations for improving diagnosis in patients presenting with diarrhoea in the community, to guide good practice to limit the spread of CDI.
Keywords: Clostridioides difficile; community; diagnosis; hospital.
Conflict of interest statement
Figures
References
-
- Suetens C, Latour K, Kärki T, Ricchizzi E, Kinross P, Moro ML, et al. The Healthcare-Associated Infections Prevalence Study Group . Prevalence of healthcare-associated infections, estimated incidence and composite antimicrobial resistance index in acute care hospitals and long-term care facilities: results from two European point prevalence surveys, 2016 to 2017. Euro Surveill. 2018;23(46):1800516. 10.2807/1560-7917.ES.2018.23.46.1800516 - DOI - PMC - PubMed
-
- Davies K, Lawrence J, Berry C, Davis G, Yu H, Cai B, et al. Risk factors for primary Clostridium difficile infection; results from the observational study of risk factors for Clostridium difficile infection in hospitalized patients with infective diarrhea (ORCHID). Front Public Health. 2020;8:293. 10.3389/fpubh.2020.00293 - DOI - PMC - PubMed
-
- Rodríguez-Pardo D, Almirante B, Bartolomé RM, Pomar V, Mirelis B, Navarro F, et al. Barcelona Clostridium difficile Study Group . Epidemiology of Clostridium difficile infection and risk factors for unfavorable clinical outcomes: results of a hospital-based study in Barcelona, Spain. J Clin Microbiol. 2013;51(5):1465-73. 10.1128/JCM.03352-12 - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources