

Tourniquet use in total knee arthroplasty and the risk of infection: a meta-analysis of randomised controlled trials
- PMID: 35776268
- PMCID: PMC9249956
- DOI: 10.1186/s40634-022-00485-9
Tourniquet use in total knee arthroplasty and the risk of infection: a meta-analysis of randomised controlled trials
Abstract
Purpose: The intra-operative use of tourniquets during Total Knee Arthroplasty (TKA) is common practice. The advantages of tourniquet use include decreased operating time and the creation of a bloodless visualisation field. However, tourniquet use has recently been linked with increased post-operative pain, reduced range of motion, and slower functional recovery. Importantly, there is limited evidence of the effect of tourniquet use on infection risk. The purpose of this systematic review and meta-analysis is to fill this gap in the literature by synthesising data pertaining to the association between tourniquet use and infection risk in TKA.
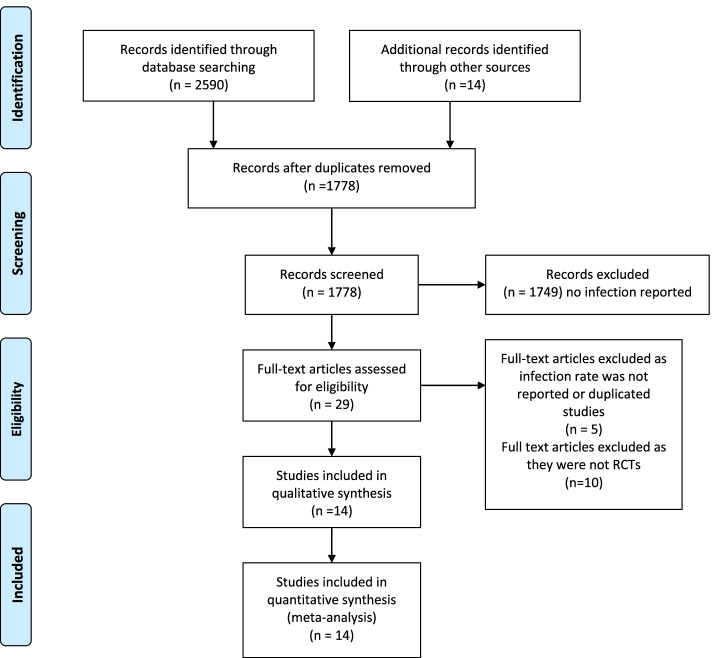
Methods: A systematic literature search was performed on Pubmed, Embase, Cochrane and clinicaltrials.gov up to May 2021. Randomized control trials were included, comparing TKA outcomes with and without tourniquet use. The primary outcome was overall infection rate. Secondary outcomes included superficial and deep infection, skin necrosis, skin blistering, DVT rate, and transfusion rate.
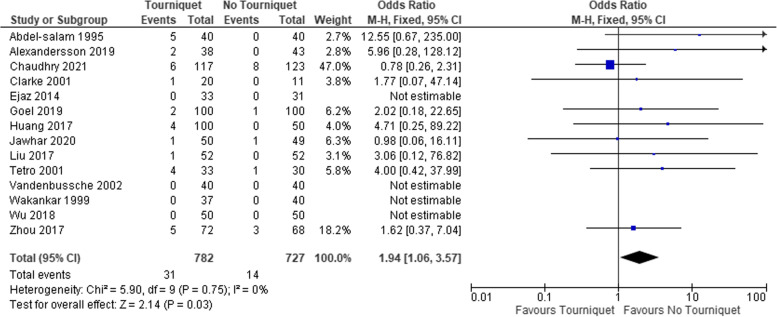
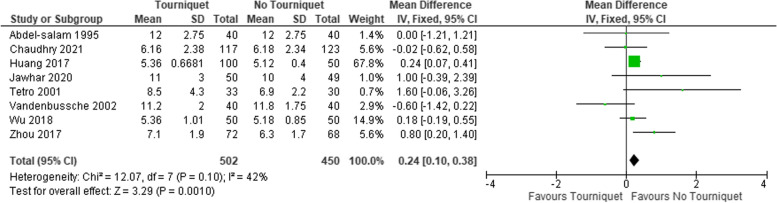
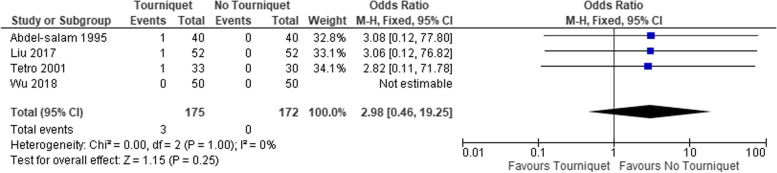
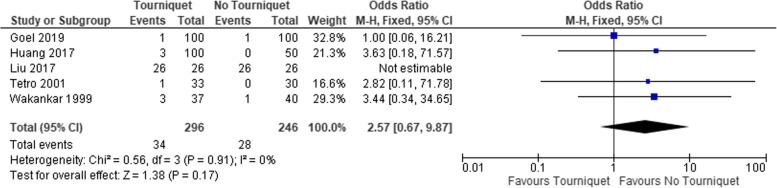
Results: 14 RCTs with 1329 patients were included. The pooled incidence of infection in the tourniquet group (4.0%, 95% CI = 2.7-5.4) was significantly higher compared to the non-tourniquet group (2.0%, 95% CI = 1.1-3.1) with an OR of 1.9 (95% CI = 1.1-3.76, p = 0.03). The length of hospital stay, haemoglobin drop (0.33 95% CI =0.12-0.54), P = 0.002) and transfusion rates (OR of 2.7, 95%CI = 1.4-5.3, P = < 0.01) were higher in the tourniquet group than the non-tourniquet group. The difference in the length of inhospital stay was 0.24 days favouring the non-tourniquet group (95% CI = 0.10-0.38, P = < 0.01). The incidence of skin blistering (OR 2.6, 95% CI = 0.7-9.9, p = 0.17), skin necrosis (OR 3.0, 95% CI = 0.50-19.3, p = 0.25), and DVT rates (OR 1.5, 95% CI = 0.60-3.60, p = 0.36) did not differ between the two groups.
Conclusion: Quantitative synthesis of the data suggested tourniquet use was associated with an increased overall risk of infection, intraoperative blood loss, need for blood transfusion and longer hospital stay. Findings of this meta-analysis do not support the routine use of tourniquet in TKA and arthroplasty surgeons should consider any potential additional risks associated with its use.
Level of evidence: meta-analysis, Level II.
Keywords: Infection; Meta-analysis; TKA; Total knee arthroplasty; Tourniquet.
© 2022. The Author(s).
Conflict of interest statement
None.
Figures

References
-
- Elkassabany NM, Cai LF, Badiola I, Kase B, Liu J, Hughes C, et al. A prospective randomized open-label study of single injection versus continuous adductor canal block for postoperative analgesia after total knee arthroplasty. Bone Joint J. 2019;101-B(3):340–347. doi: 10.1302/0301-620X.101B3.BJJ-2018-0852.R2. - DOI - PubMed
-
- Greco NJ, Manocchio AG, Lombardi A, v., Gao SL, Adams J, Berend KR. Should postoperative haemoglobin and potassium levels be checked routinely following blood-conserving primary total joint arthroplasty? Bone Joint J. 2019;101-B(1_Supple_A):25–31. doi: 10.1302/0301-620X.101B1.BJJ-2018-0554.R1. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
