

Risk factors of clinically relevant postoperative pancreatic fistula after pancreaticoduodenectomy: A systematic review and meta-analysis
- PMID: 35776984
- PMCID: PMC9239615
- DOI: 10.1097/MD.0000000000029757
Risk factors of clinically relevant postoperative pancreatic fistula after pancreaticoduodenectomy: A systematic review and meta-analysis
Abstract
Background: Clinically relevant postoperative pancreatic fistula (CR-POPF) is a common and troublesome complication after pancreatoduodenectomy (PD). We conducted a systematic review and meta-analysis to identify the risk factors of CR-POPF after PD.
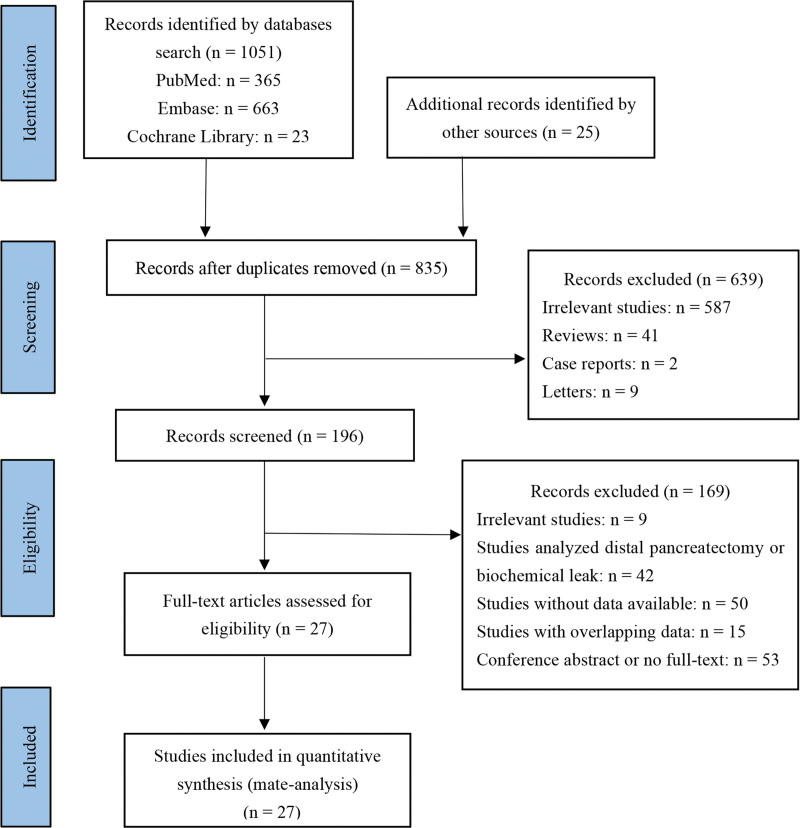
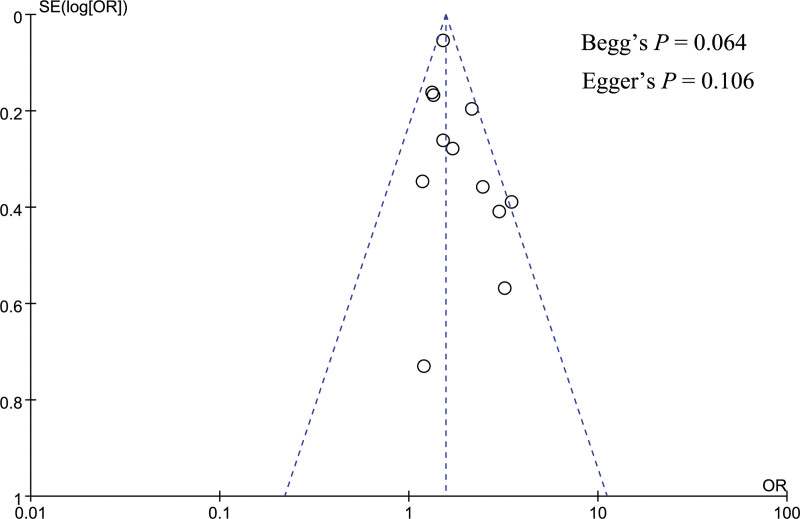
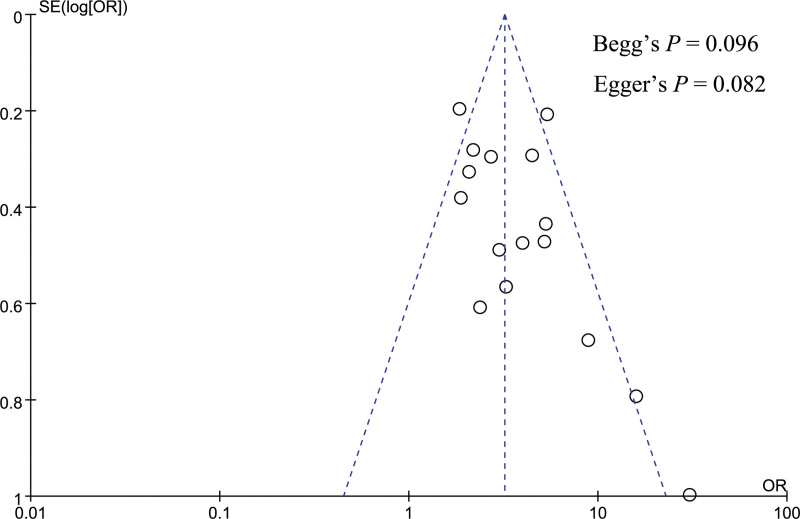
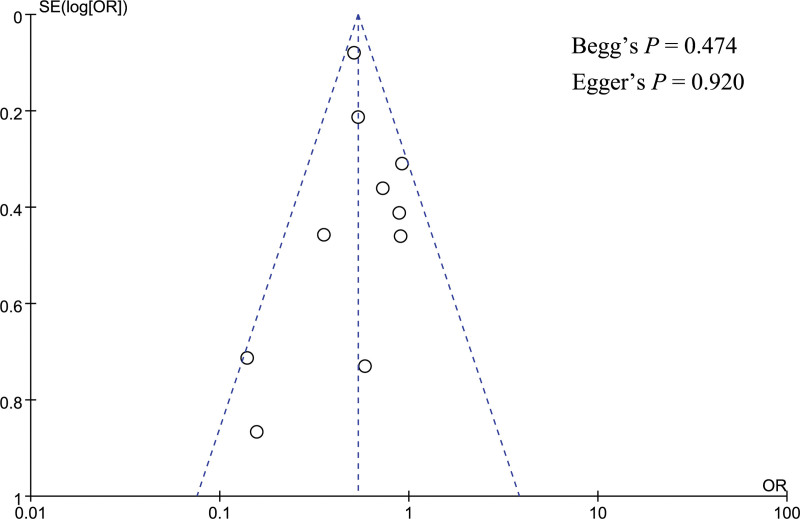
Methods: We searched PubMed, EMBASE, and Cochrane Library databases for studies related to risk factors of CR-POPF after PD. Odds ratios (ORs) with corresponding 95% confidence intervals (CIs) were extracted from the included studies, then a meta-analysis was conducted. If necessary, sensitivity analysis would be performed by changing the effect model or excluding 1 study at a time. Publication bias was assessed by funnel plot and Begg test and Egger test.
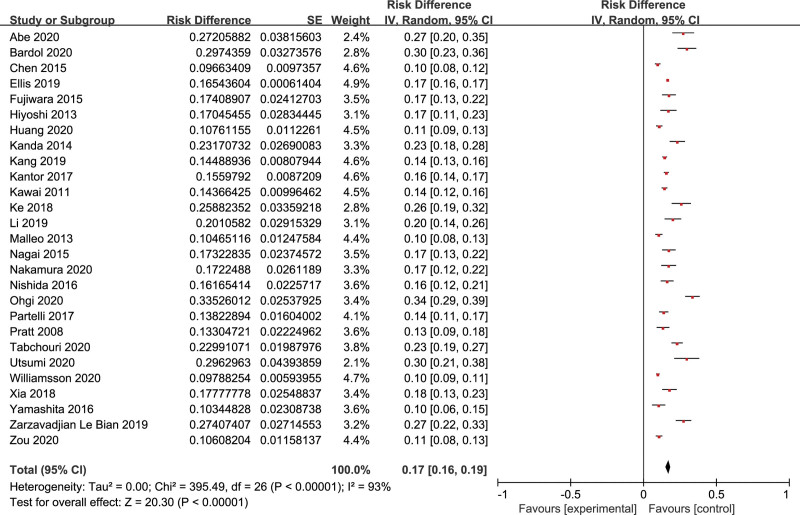
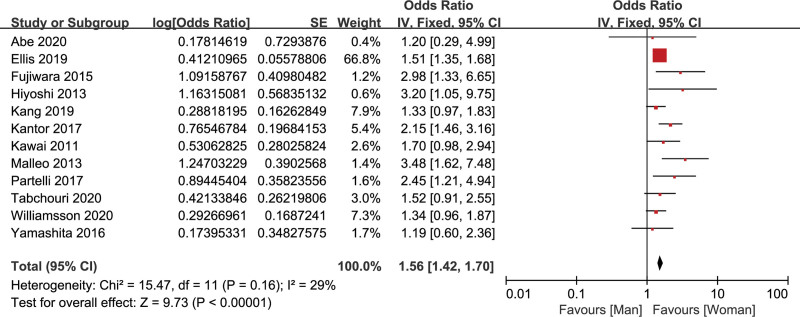
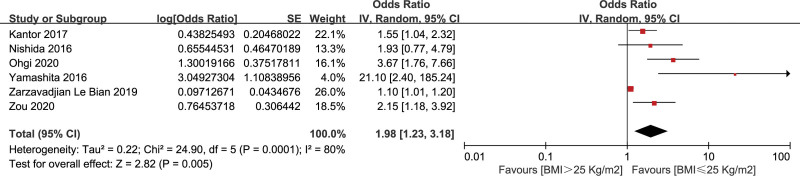
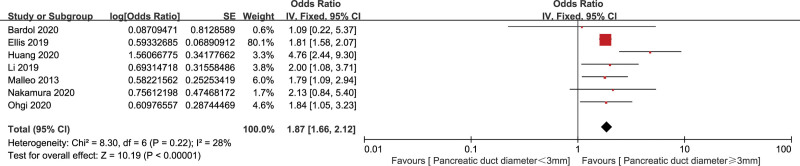
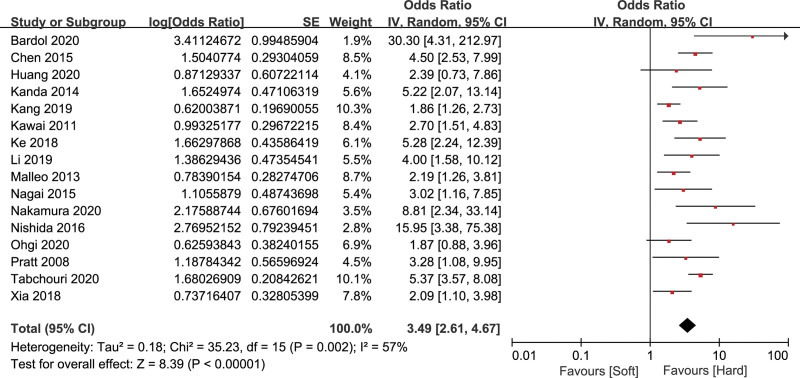
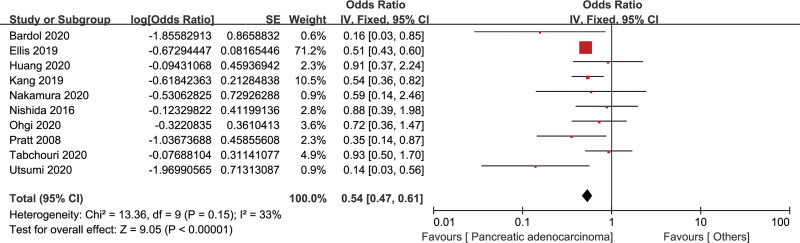
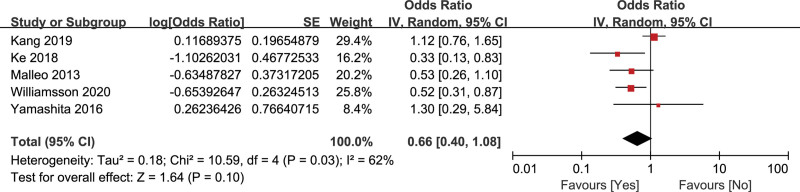
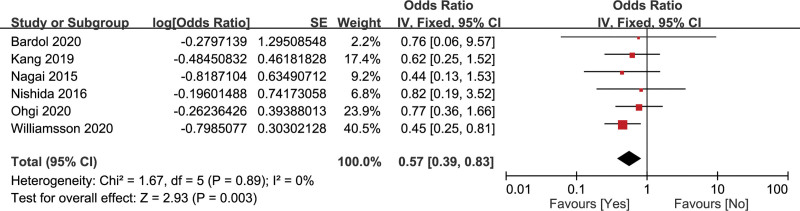
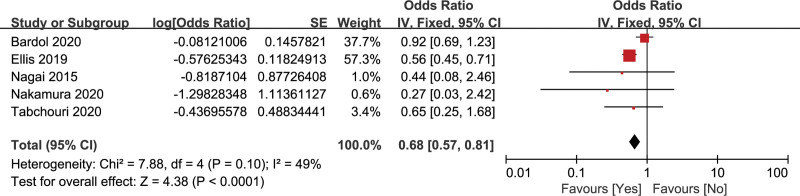
Results: A total of 27 studies with 24,740 patients were included, and CR-POPF occurred in 3843 patients (incidence = 17%, 95% CI: 16%-19%). Male (OR = 1.56, 95% CI: 1.42-1.70), body mass index >25 kg/m2 (OR = 1.98, 95% CI: 1.23-3.18), pancreatic duct diameter <3 mm (OR = 1.87, 95% CI: 1.66-2.12), soft pancreatic texture (OR = 3.49, 95% CI: 2.61-4.67), and blood transfusion (OR = 3.10, 95% CI: 2.01-4.77) can significantly increase the risk of CR-POPF. Pancreatic adenocarcinoma (OR = 0.54, 95% CI: 0.47-0.61), vascular resection (OR = 0.57, 95% CI: 0.39-0.83), and preoperative chemoradiotherapy (OR = 0.68, 95% CI: 0.57-0.81) can significantly decrease the factor of CR-POPF. Diabetes mellitus was not statistically associated with CR-POPF (OR = 0.66, 95% CI: 0.40-1.08). However, the analysis of body mass index, pancreatic texture, and diabetes mellitus had a high heterogeneity, then sensitivity analysis was performed, and the result after sensitivity analysis showed diabetes mellitus can significantly decrease the risk of CR-POPF. There was no significant publication bias in this meta-analysis.
Conclusions: The current review assessed the effects of different factors on CR-POPF. This can provide a basis for the prevention and management of CR-POPF. Effective interventions targeting the above risk factors should be investigated in future studies for decreasing the occurrence of CR-POPF.
Copyright © 2022 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures

References
-
- Ausania F, Landi F, Martinez-Perez A, et al. A meta-analysis of randomized controlled trials comparing laparoscopic vs open pancreaticoduodenectomy. HPB (Oxford). 2019;21:1613–20. - PubMed
-
- Allen PJ, Gönen M, Brennan MF, et al. Pasireotide for postoperative pancreatic fistula. N Engl J Med. 2014;370:2014–22. - PubMed
-
- Bassi C, Marchegiani G, Dervenis C, et al. The 2016 update of the international study group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 years after. Surgery. 2017;161:584–91. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
